

SHARP hypofractionated stereotactic radiotherapy is well tolerated in prostate cancer : Toxicity and quality of life assessment
- PMID: 27221312
- PMCID: PMC4919372
- DOI: 10.1007/s00066-016-0971-2
SHARP hypofractionated stereotactic radiotherapy is well tolerated in prostate cancer : Toxicity and quality of life assessment
Abstract
Background: Quality of life (QoL) is one of the most significant issues in prostate cancer treatment decisions. This study aimed to investigate the toxicity of hypofractionated stereotactic radiotherapy (SBRT) and QoL after treatment in localized prostate cancer patients.
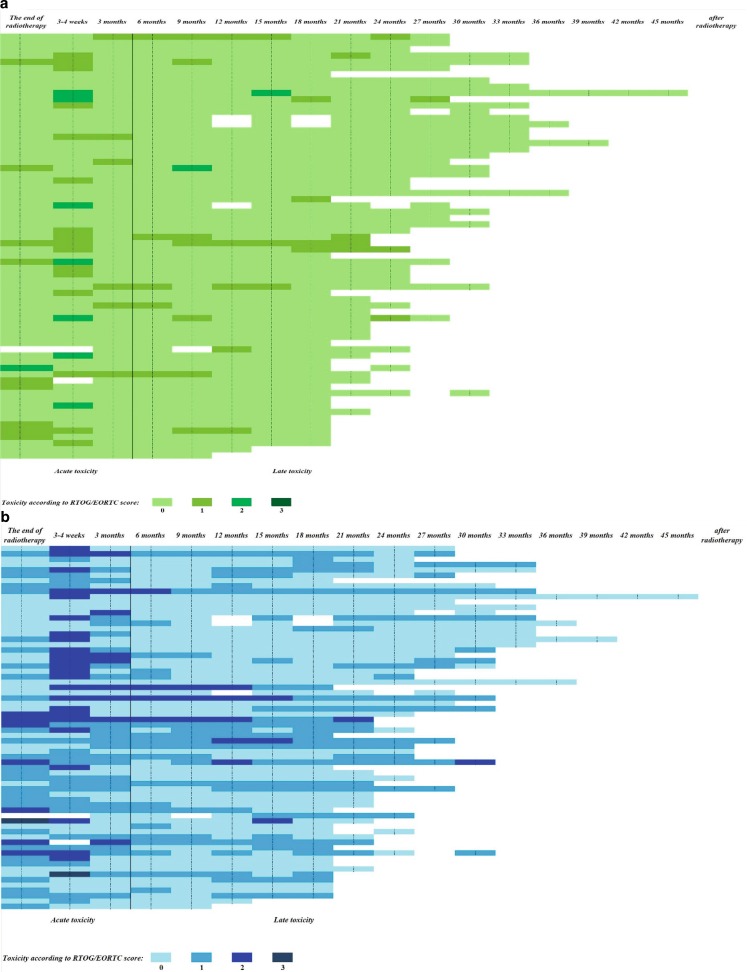
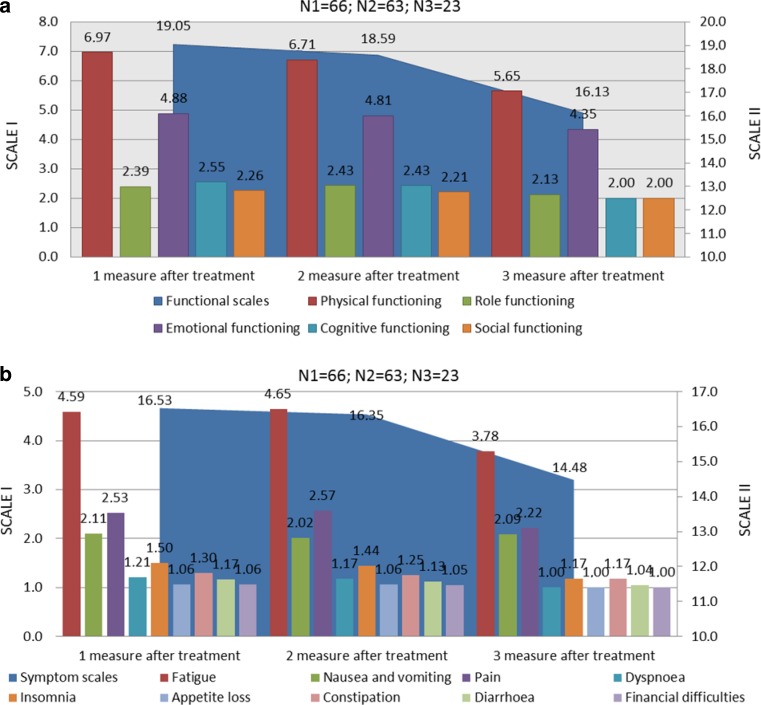
Materials and methods: A prospective single-center clinical study was performed in low- and intermediate-risk prostate cancer patients. Patients received 33.5 Gy in 5 fractions (SHARP regimen). Acute and late toxicity was assessed according to RTOG/EORTC score. Patients filled out EORTC QLQ-C30 and prostate cancer-specific QLQ-PR25 questionnaires.
Results: The analysis included 68 prostate cancer patients (55-83 years, median 73) with clinical stage T1c-T2cN0M0, median combined Gleason score of 6 (3-8), and median prostate-specific antigen (PSA) level of 10 ng/mL (4-20 ng/mL). Neoadjuvant androgen deprivation therapy was given to 52 patients (76.5 %), and stopped in 31 patients (45.5 %) after 6 months; in 21 patients (31 %) after 2-3 years. Average and median follow-up was 24 months (18-45). Median nadir PSA level was 0.03 ng/mL for all patients and 0.6 ng/mL for patients without hormone treatment. No patients had PSA failure. There were no acute grade IV toxicities. One patient (1.5 %) developed grade III and 24 patients (35.3 %) grade II acute bladder toxicity. No one developed grade III and 7 patients (10.3 %) grade II acute rectal toxicity. No grade III or IV late gastrointestinal or genitourinary toxicities were reported. Grade II late urinary symptoms were observed in 8 patients (11.8 %) and gastrointestinal symptoms in 3 patients (4.4 %). Global health status/QoL was good and improved during the observational period.
Conclusion: SBRT for prostate cancer patients is a well-tolerated treatment in terms of toxicity and QoL, has no negative impact on functioning and everyday life, with the important benefit of a short treatment period. However, long-term follow-up data are needed.
Hintergrund: Die Lebensqualität (QoL) ist zu einem der wichtigsten Schwerpunkte bei der Wahl der Prostatakarzinombehandlung geworden. Das Thema dieser Studie war die Untersuchung der Toxizität der hypofraktionierten stereotaktischen Radiotherapie (SBRT) und der QoL nach Behandlung des lokal begrenzten Prostatakarzinoms.
Materialien und Methoden: Die prospektive, monozentrische, klinische Studie wurde bei Prostatakarzinompatienten mit niedrigem bis mittlerem Risiko durchgeführt. Die Patienten erhielten 33,5 Gy in 5 Fraktionen (SHARP-Behandlungsschema). Akute und späte Toxizität wurden nach den Kriterien des RTOG/EORTC-Scores klassifiziert. Die Patienten füllten das EORTC-QLQ-C30- und das prostatakarzinomspezifische QLQ-PR25-Formular aus.
Ergebnisse: Die Analyse umfasste 68 Prostatakarzinompatienten (medianes Alter 73, Spanne 55–83 Jahre) im klinischen Staging T1c–T2cN0M0, mit einem medianen Gleason-Score von 6 (Spanne 3–8) und einem medianen PSA-Wert (prostataspezifisches Antigen) von 10 ng/ml (Spanne 4–20 ng/ml). Eine neoadjuvante Androgendeprivationstherapie erhielten 52 Patienten (76,5 %); die Hormontherapie beendet 31 Patienten (45,5 %) nach 6 Monaten und 21 Patienten (31 %) nach 2–3 Jahren. Das durchschnittliche und mediane Follow-up dauerte 24 Monate (Spanne 18–45). Der mediane PSA-Nadir betrug 0,03 ng/ml für alle Patienten und 0,6 ng/ml für Patienten ohne Hormontherapie. PSA-Versagen und akute Grad-IV-Toxizitäten traten nicht auf. Ein Patient (1,5 %) hatte eine Grad-III- und 24 Patienten (35,3 %) eine Grad-II-Harnblasentoxizität, kein Patient eine Grad-III- und 7 Patienten (10,3 %) eine akute Grad-II-Rektumtoxizität. Späte gastrointestinale oder urogenitale Toxizitäten III. oder IV. Grades wurden nicht berichtet. Bei 8 Patienten (11,8 %) traten späte Miktionsbeschwerden II. Grades und bei 3 Patienten (4,4 %) gastrointestinale Symptome auf. Globaler Gesundheitsstatus/QoL war gut und besserte sich in der untersuchten Zeit.
Schlussfolgerung: SBRT ist beim Prostatakarzinom eine gut tolerierte Behandlung hinsichtlich Toxizität und QoL, ohne negativen Einfluss auf das Alltagsleben und dem wichtigen Vorteil einer kurzen Behandlungszeit. Langfristige Follow-up-Untersuchungen müssen noch folgen.
Keywords: Bladder; Hypofractionated stereotactic radiotherapy; Organs of risk; Quality of Life; Rectum.
Figures
Similar articles
-
Early Tolerance and Tumor Control Outcomes with High-dose Ultrahypofractionated Radiation Therapy for Prostate Cancer.Eur Urol Oncol. 2020 Dec;3(6):748-755. doi: 10.1016/j.euo.2019.09.006. Epub 2019 Oct 23. Eur Urol Oncol. 2020. PMID: 31668713 Free PMC article. Clinical Trial.
-
Stereotactic body radiotherapy for localized prostate cancer: interim results of a prospective phase II clinical trial.Int J Radiat Oncol Biol Phys. 2009 Mar 15;73(4):1043-8. doi: 10.1016/j.ijrobp.2008.05.059. Epub 2008 Aug 26. Int J Radiat Oncol Biol Phys. 2009. PMID: 18755555 Clinical Trial.
-
Five-Year Outcomes of a Phase 1 Dose-Escalation Study Using Stereotactic Body Radiosurgery for Patients With Low-Risk and Intermediate-Risk Prostate Cancer.Int J Radiat Oncol Biol Phys. 2019 May 1;104(1):42-49. doi: 10.1016/j.ijrobp.2018.12.045. Epub 2019 Jan 4. Int J Radiat Oncol Biol Phys. 2019. PMID: 30611838 Free PMC article. Clinical Trial.
-
Prostate Stereotactic Body Radiation Therapy: An Overview of Toxicity and Dose Response.Int J Radiat Oncol Biol Phys. 2021 May 1;110(1):237-248. doi: 10.1016/j.ijrobp.2020.09.054. Epub 2020 Dec 22. Int J Radiat Oncol Biol Phys. 2021. PMID: 33358229 Free PMC article.
-
Genitourinary toxicity in patients receiving TURP prior to hypofractionated radiotherapy for clinically localized prostate cancer: A scoping review.Urol Oncol. 2024 Jun;42(6):165-174. doi: 10.1016/j.urolonc.2024.02.011. Epub 2024 Mar 19. Urol Oncol. 2024. PMID: 38503591
Cited by
-
Hypofractionated Radiation Therapy for Localized Prostate Cancer: An ASTRO, ASCO, and AUA Evidence-Based Guideline.J Clin Oncol. 2018 Oct 11;36(34):JCO1801097. doi: 10.1200/JCO.18.01097. Online ahead of print. J Clin Oncol. 2018. PMID: 30307776 Free PMC article. No abstract available.
-
Volumetric modulated arc therapy (VMAT): a review of clinical outcomes-what is the clinical evidence for the most effective implementation?Br J Radiol. 2022 Aug 1;95(1136):20201289. doi: 10.1259/bjr.20201289. Epub 2022 Jul 4. Br J Radiol. 2022. PMID: 35616646 Free PMC article. Review.
-
Hypo-fractionated SBRT for localized prostate cancer: a German bi-center single treatment group feasibility trial.Radiat Oncol. 2017 Aug 18;12(1):138. doi: 10.1186/s13014-017-0872-2. Radiat Oncol. 2017. PMID: 28821268 Free PMC article. Clinical Trial.
-
Rectal/urinary toxicity after hypofractionated vs conventional radiotherapy in low/intermediate risk localized prostate cancer: systematic review and meta analysis.Oncotarget. 2017 Mar 7;8(10):17383-17395. doi: 10.18632/oncotarget.14798. Oncotarget. 2017. PMID: 28129649 Free PMC article.
-
Tumor Control Probability Modeling and Systematic Review of the Literature of Stereotactic Body Radiation Therapy for Prostate Cancer.Int J Radiat Oncol Biol Phys. 2021 May 1;110(1):227-236. doi: 10.1016/j.ijrobp.2020.08.014. Epub 2020 Sep 6. Int J Radiat Oncol Biol Phys. 2021. PMID: 32900561 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
