

Improving Adherence to Post-Cervical Biopsy Sexual Abstinence in Kenyan Female Sex Workers
- PMID: 27221472
- PMCID: PMC5089664
- DOI: 10.1111/aji.12520
Improving Adherence to Post-Cervical Biopsy Sexual Abstinence in Kenyan Female Sex Workers
Abstract
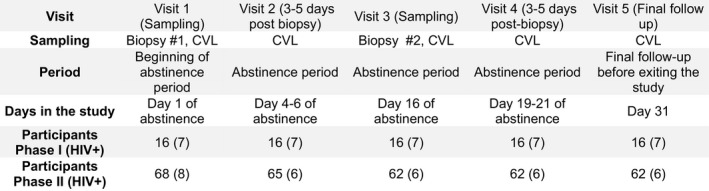
Problem: Cervical biopsies offer a unique opportunity for studying local immune response. To investigate hormonally induced immune fluctuations in cervical tissues of Kenyan female sex workers, we improved biopsy sampling protocol safety. Here, we report on steps taken to minimize exposure to HIV following two cervical biopsies.
Methods of study: Women were asked to abstain from vaginal intercourse to limit HIV exposure during wound healing with financial compensation. A comprehension tool for informed consent, on-site detection of prostate-specific antigens indicating unprotected intercourse within 48 hr, and bi-weekly text message reminders were implemented.
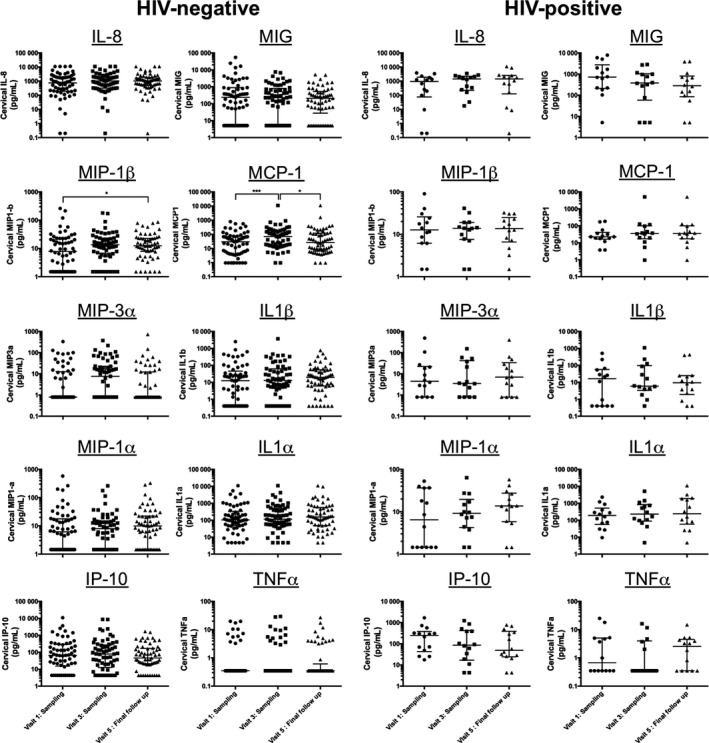
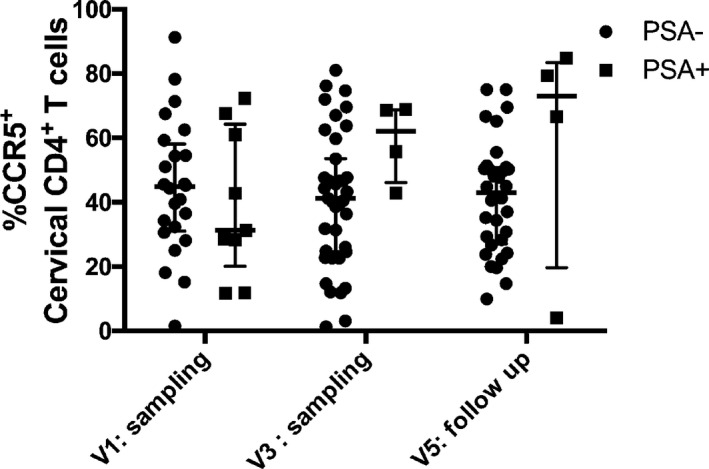
Results: The implemented methods improved compliance with post-procedure abstinence by two times (P = 0.013). Fourteen days following a cervical biopsy, no sign of genital inflammation or change in HIV T-cell target proportion were observed.
Conclusions: This study provides new tools for limiting HIV exposure in studies requiring biopsy sampling among women at risk of acquiring HIV.
Keywords: Female genital tract; HIV; immunology; mucosal; prostate-specific antigens; safety.
© 2016 The Authors. American Journal of Reproductive Immunology Published by John Wiley & Sons Ltd.
Figures

Similar articles
-
Feasibility and safety of cervical biopsy sampling for mucosal immune studies in female sex workers from Nairobi, Kenya.PLoS One. 2012;7(10):e47570. doi: 10.1371/journal.pone.0047570. Epub 2012 Oct 15. PLoS One. 2012. PMID: 23077640 Free PMC article.
-
HIV-1-specific mucosal IgA in a cohort of HIV-1-resistant Kenyan sex workers.AIDS. 1999 Jan 14;13(1):23-9. doi: 10.1097/00002030-199901140-00004. AIDS. 1999. PMID: 10207541
-
Increased Cervical CD4+CCR5+ T Cells Among Kenyan Sex Working Women Using Depot Medroxyprogesterone Acetate.AIDS Res Hum Retroviruses. 2019 Mar;35(3):236-246. doi: 10.1089/AID.2018.0188. Epub 2019 Jan 24. AIDS Res Hum Retroviruses. 2019. PMID: 30585733 Free PMC article.
-
Voluntary medical male circumcision for HIV prevention and early resumption of sexual activity: a literature review.AIDS Care. 2015;27(8):986-9. doi: 10.1080/09540121.2015.1017797. Epub 2015 Mar 4. AIDS Care. 2015. PMID: 25738780 Review.
-
Preventing HIV infection without targeting the virus: how reducing HIV target cells at the genital tract is a new approach to HIV prevention.AIDS Res Ther. 2017 Sep 12;14(1):46. doi: 10.1186/s12981-017-0166-7. AIDS Res Ther. 2017. PMID: 28893304 Free PMC article. Review.
Cited by
-
HIV-Exposed Seronegative Sex Workers Express Low T-Cell Activation and an Intact Ectocervical Tissue Microenvironment.Vaccines (Basel). 2021 Mar 4;9(3):217. doi: 10.3390/vaccines9030217. Vaccines (Basel). 2021. PMID: 33806390 Free PMC article.
-
Distinct cervical tissue-adherent and luminal microbiome communities correlate with mucosal host gene expression and protein levels in Kenyan sex workers.Microbiome. 2023 Mar 31;11(1):67. doi: 10.1186/s40168-023-01502-4. Microbiome. 2023. PMID: 37004130 Free PMC article.
-
Women for science and science for women: Gaps, challenges and opportunities towards optimizing pre-exposure prophylaxis for HIV-1 prevention.Front Immunol. 2022 Dec 6;13:1055042. doi: 10.3389/fimmu.2022.1055042. eCollection 2022. Front Immunol. 2022. PMID: 36561760 Free PMC article. Review.
-
Estradiol-mediated enhancement of the human ectocervical epithelial barrier correlates with desmoglein-1 expression in the follicular menstrual phase.Front Endocrinol (Lausanne). 2024 Oct 8;15:1454006. doi: 10.3389/fendo.2024.1454006. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 39439565 Free PMC article.
-
Sustained immune activation and impaired epithelial barrier integrity in the ectocervix of women with chronic HIV infection.PLoS Pathog. 2024 Nov 19;20(11):e1012709. doi: 10.1371/journal.ppat.1012709. eCollection 2024 Nov. PLoS Pathog. 2024. PMID: 39561211 Free PMC article.
References
-
- McKinnon LR, Nyanga B, Chege D, Izulla P, Kimani M, Huibner S, Gelmon L, Block KE, Cicala C, Anzala AO, Arthos J, Kimani J, Kaul R: Characterization of a human cervical CD4+ T cell subset coexpressing multiple markers of HIV susceptibility. J Immunol 2011; 187:6032–6042. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
