

Cardiovascular MRI with ferumoxytol
- PMID: 27221526
- PMCID: PMC10202101
- DOI: 10.1016/j.crad.2016.03.020
Cardiovascular MRI with ferumoxytol
Abstract
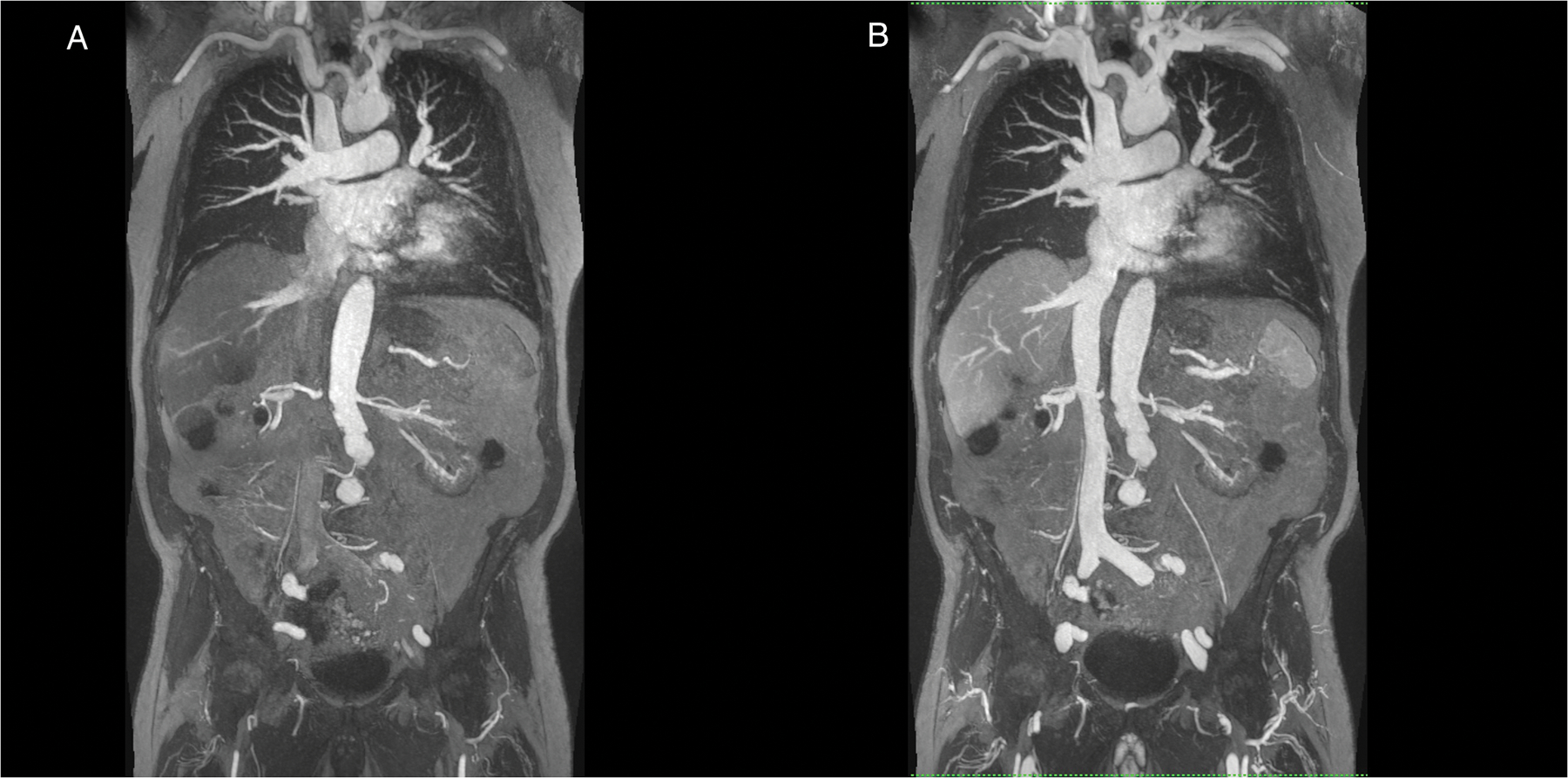
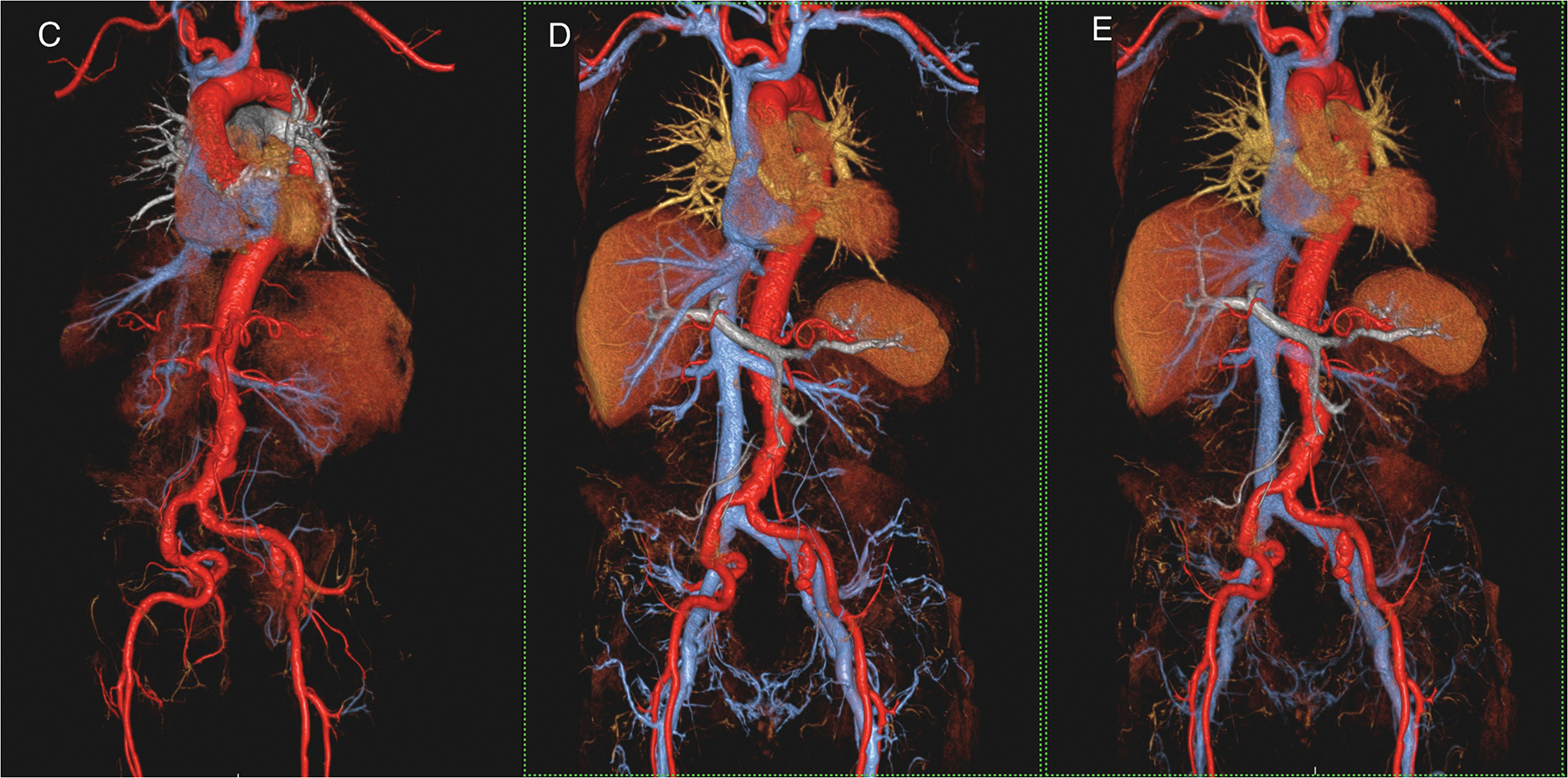
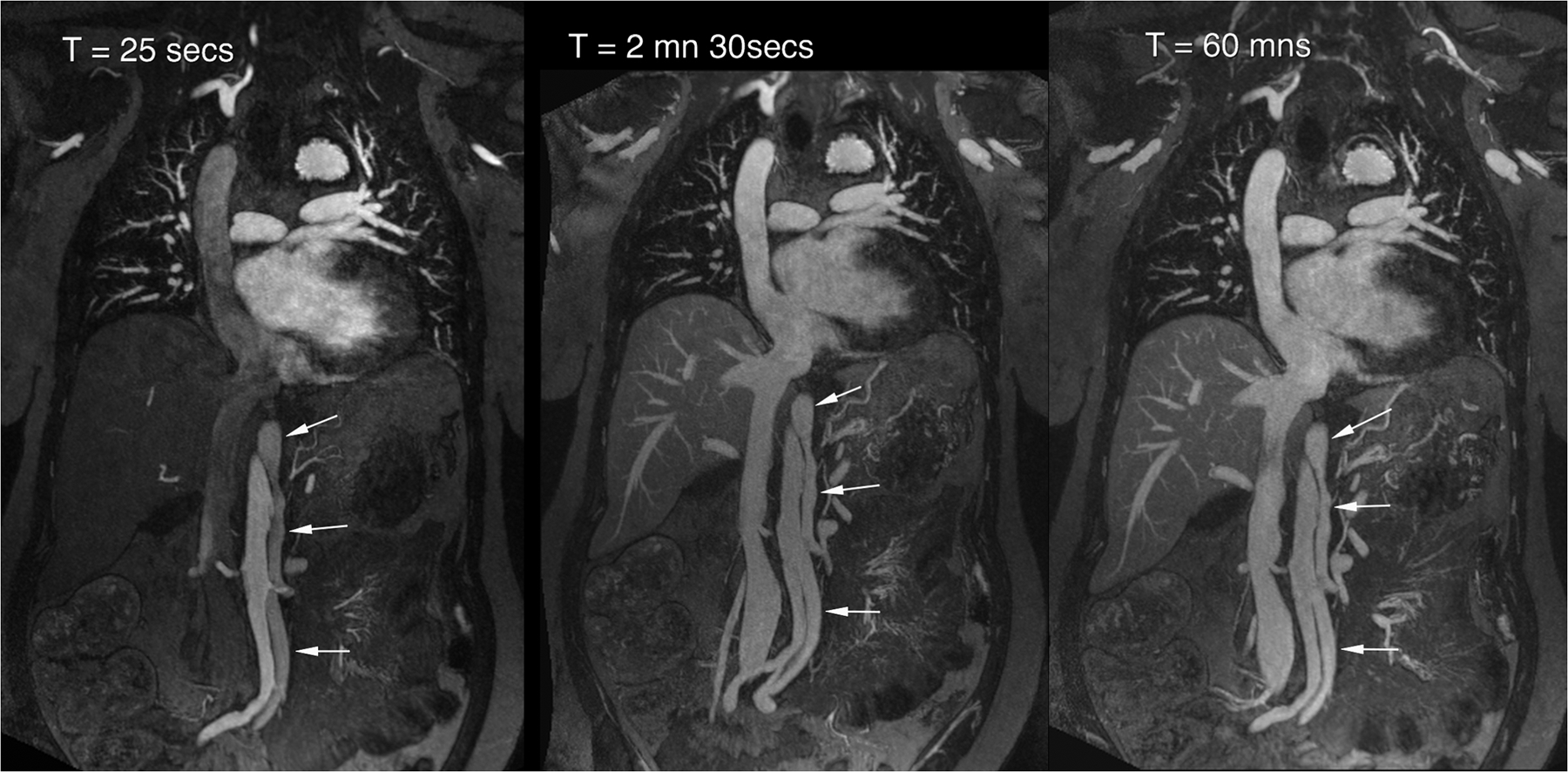
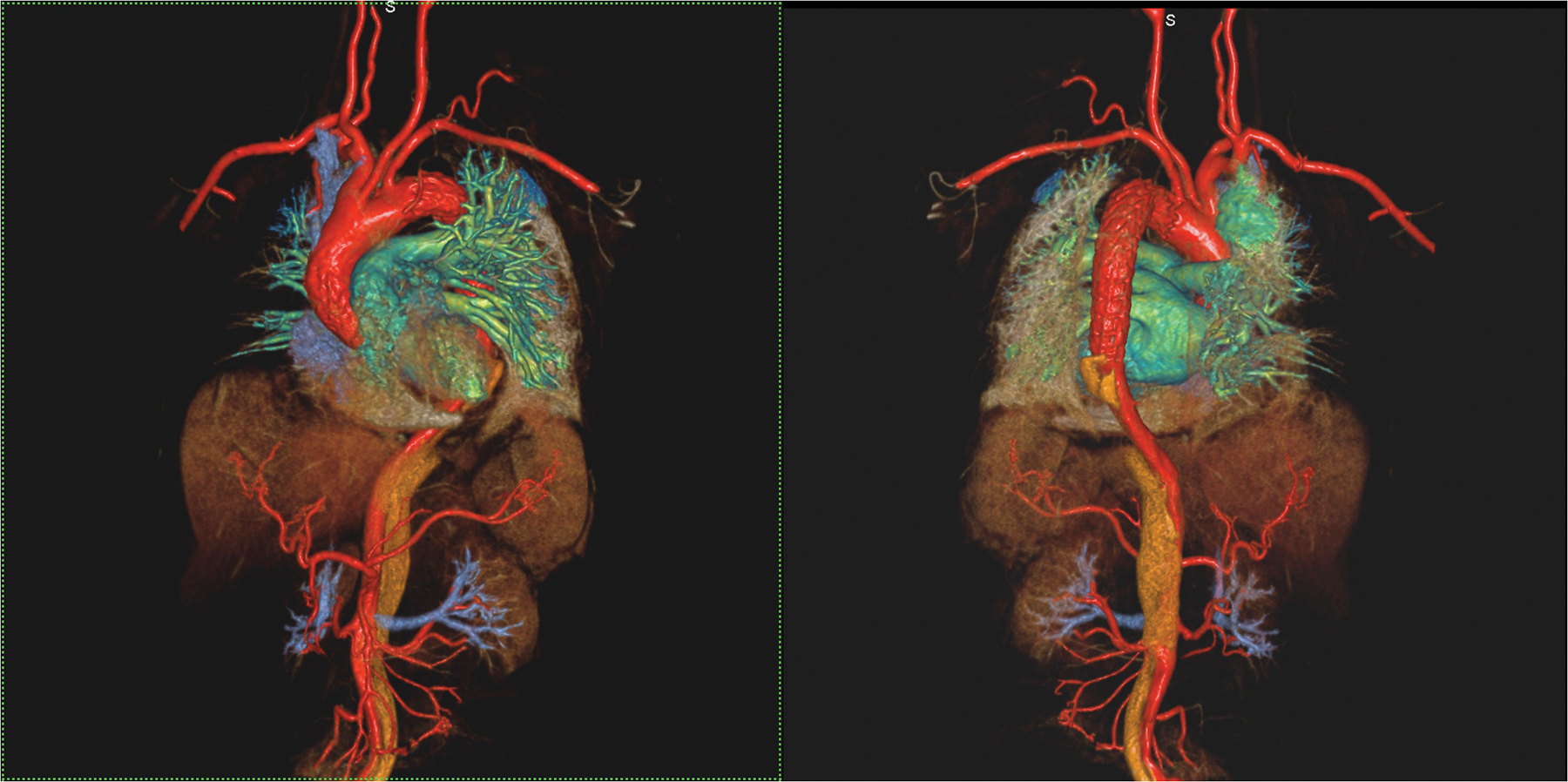
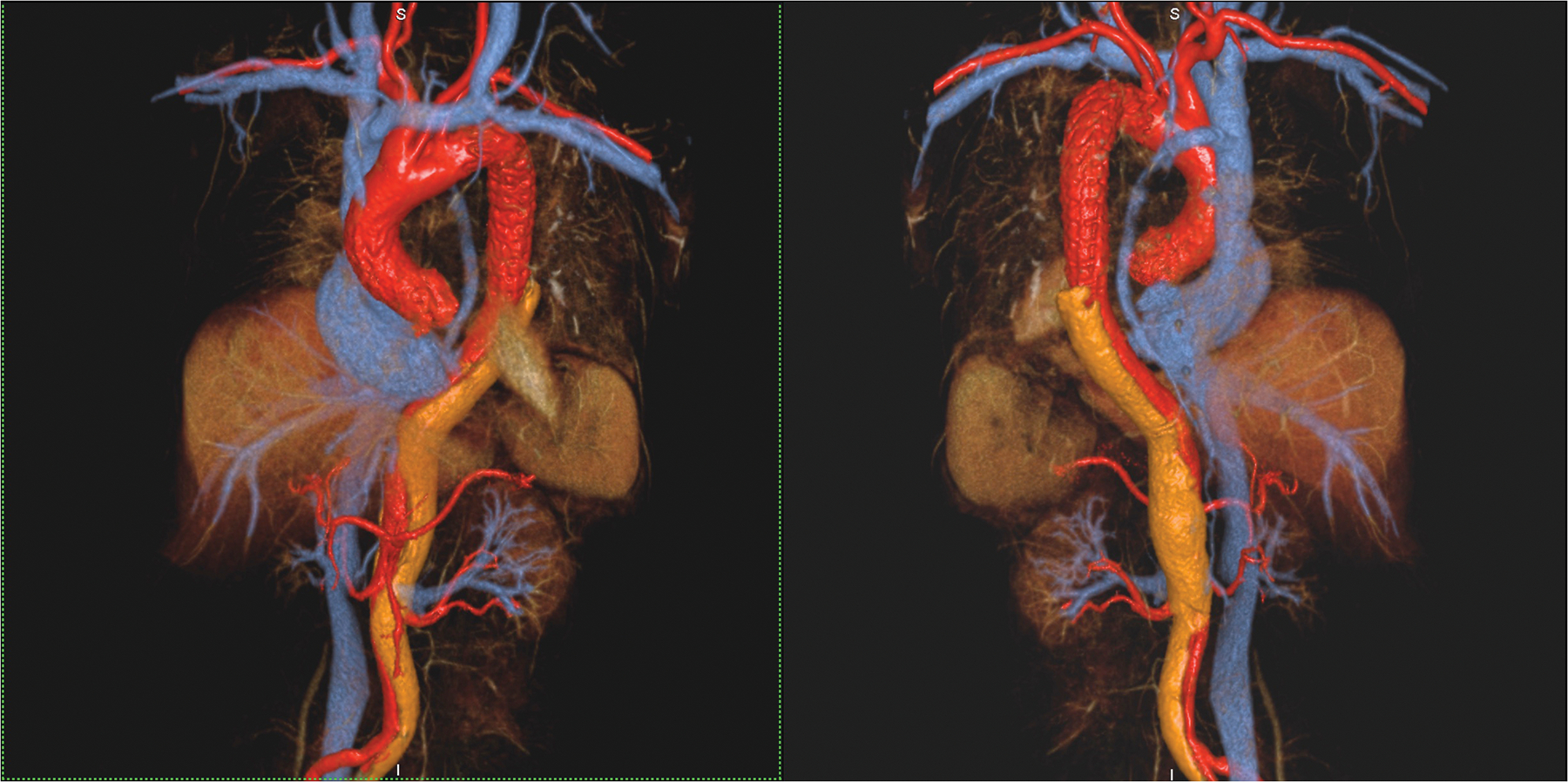
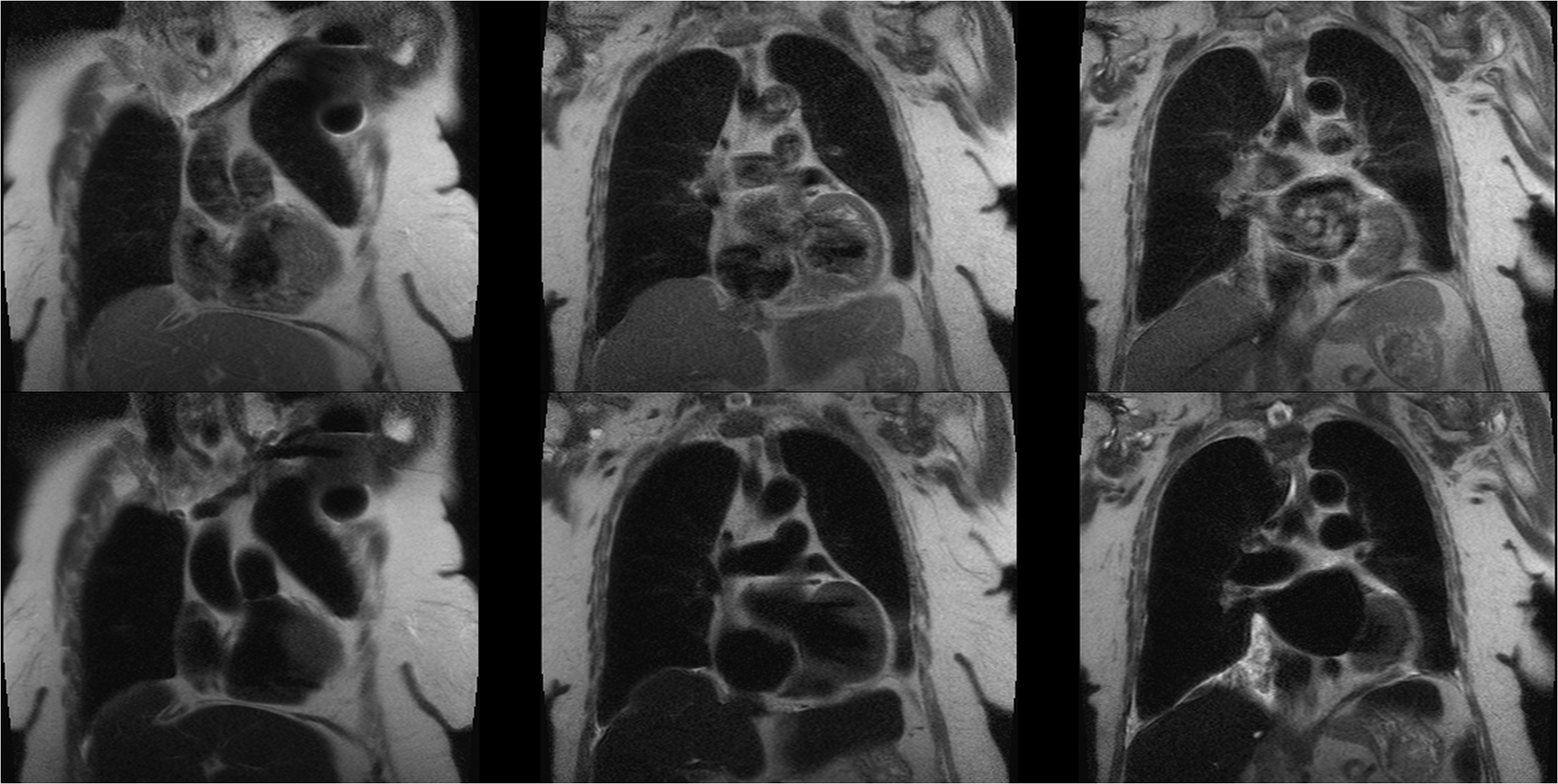
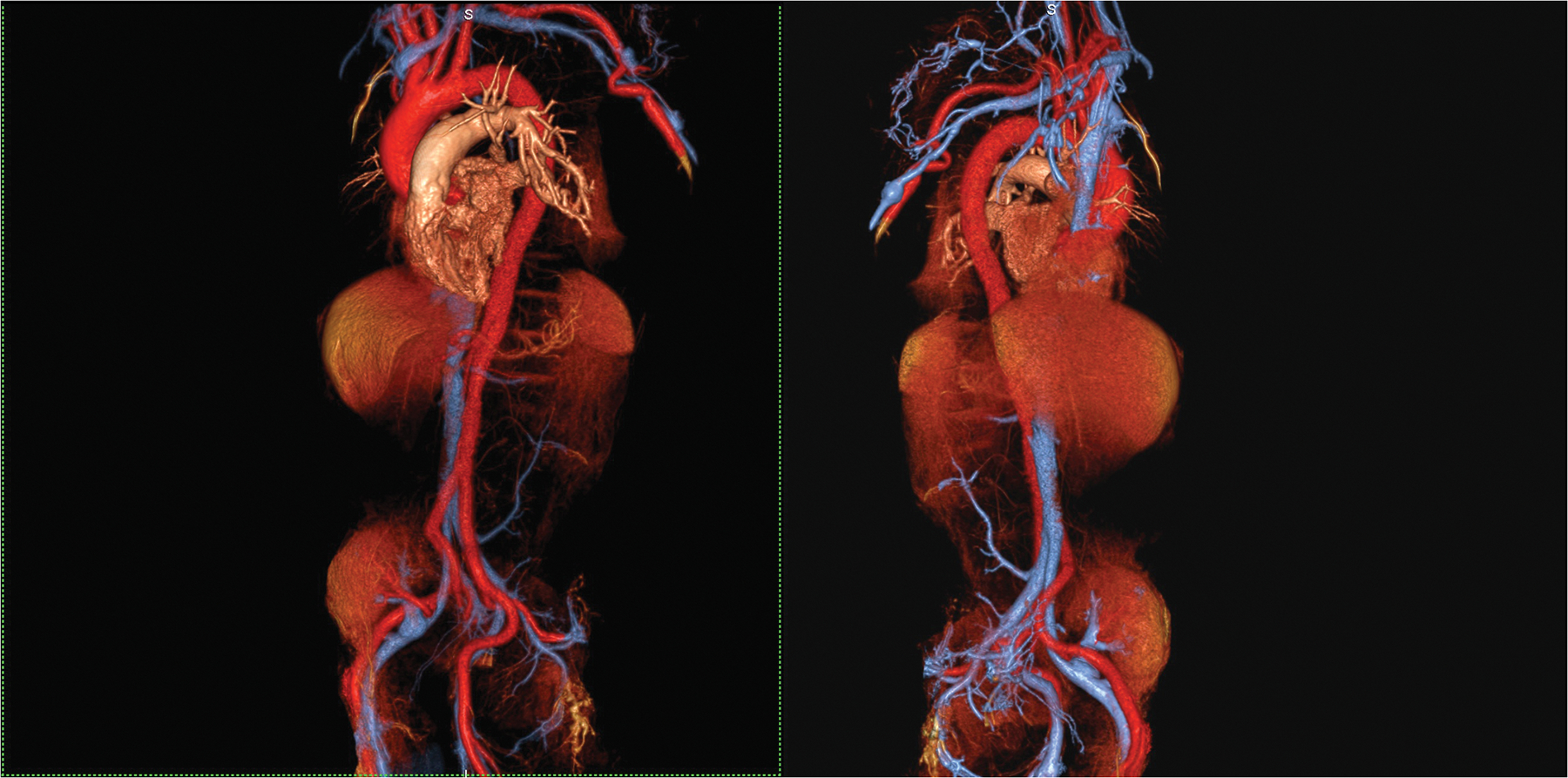
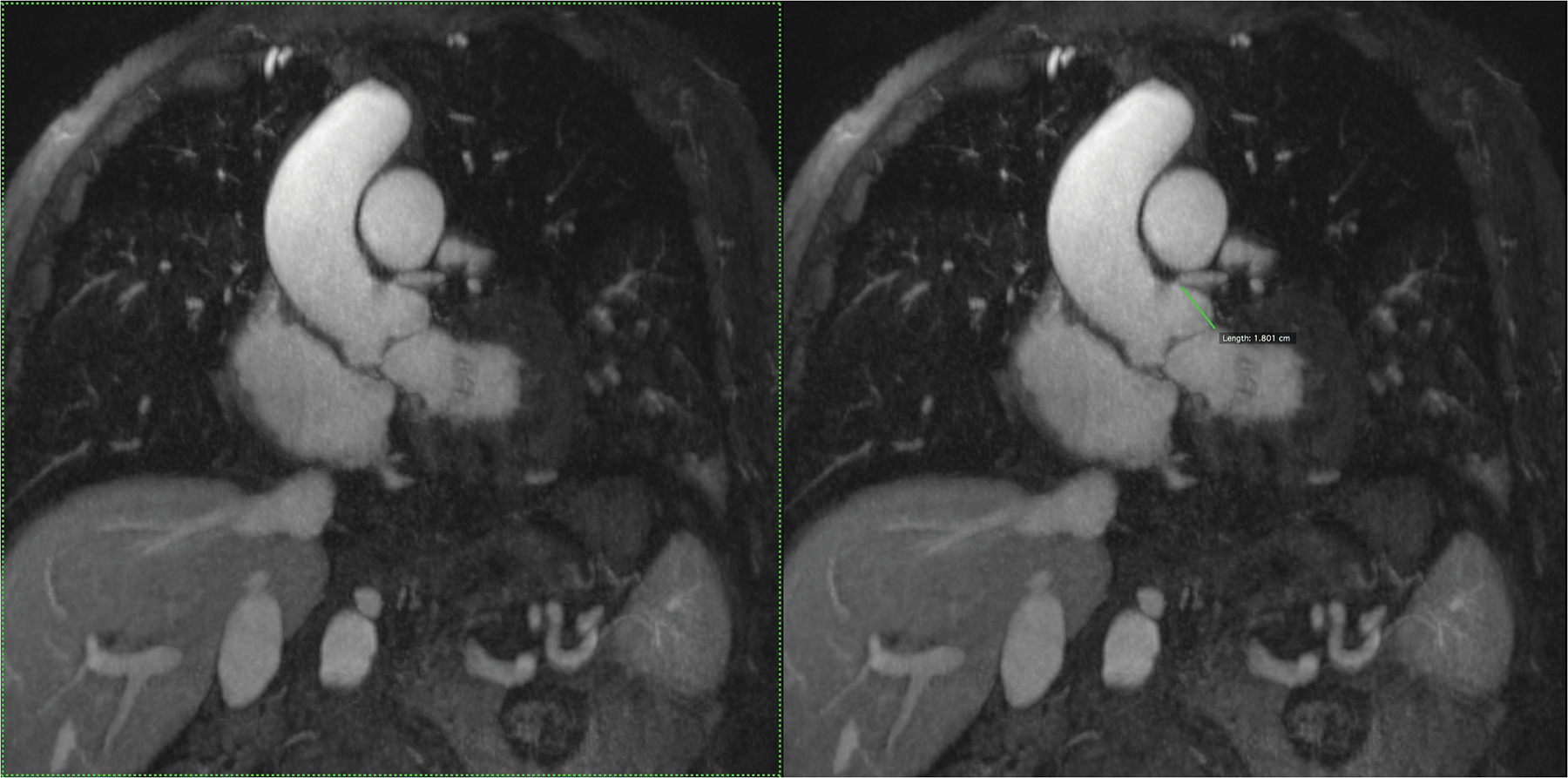
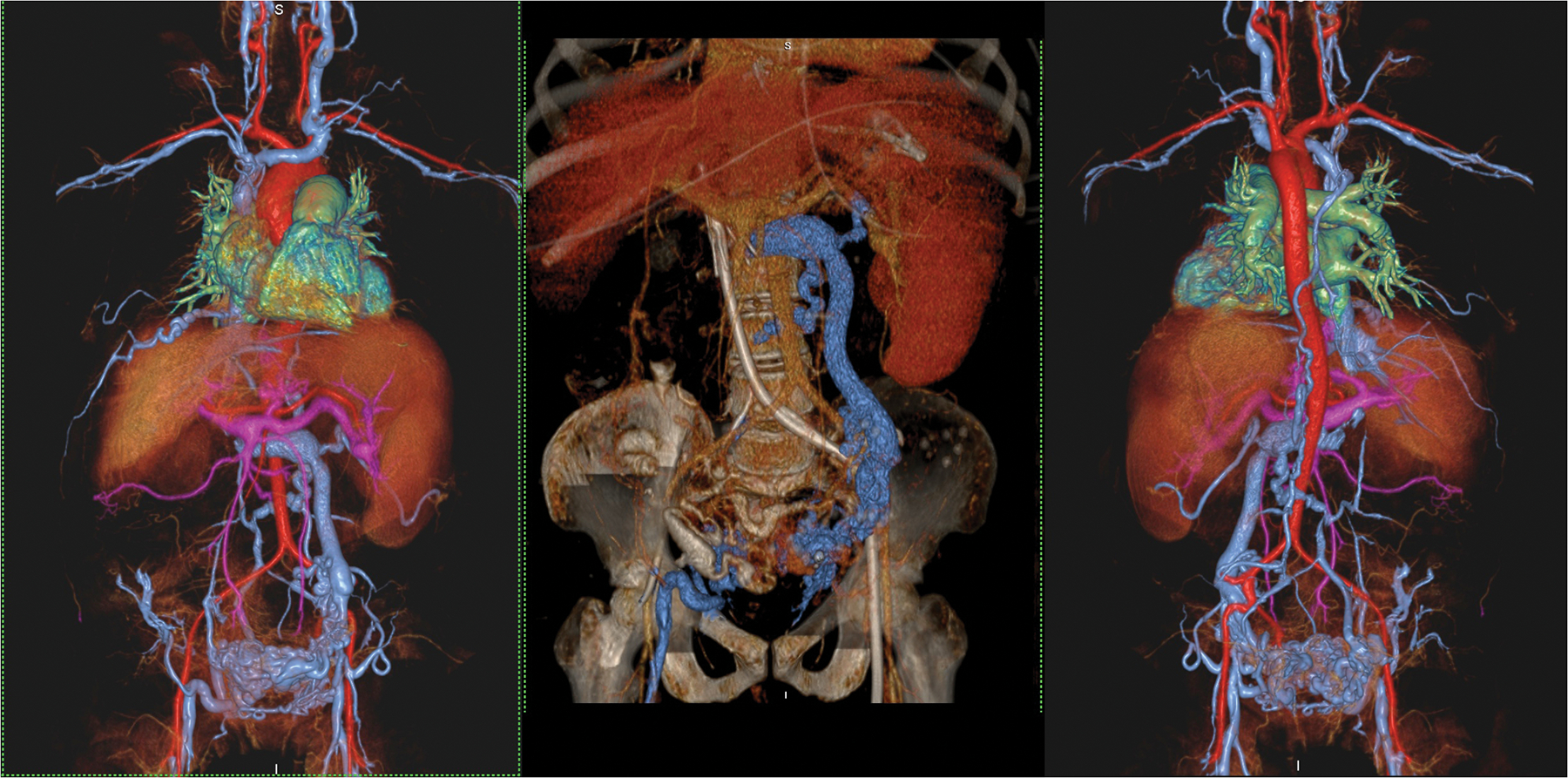
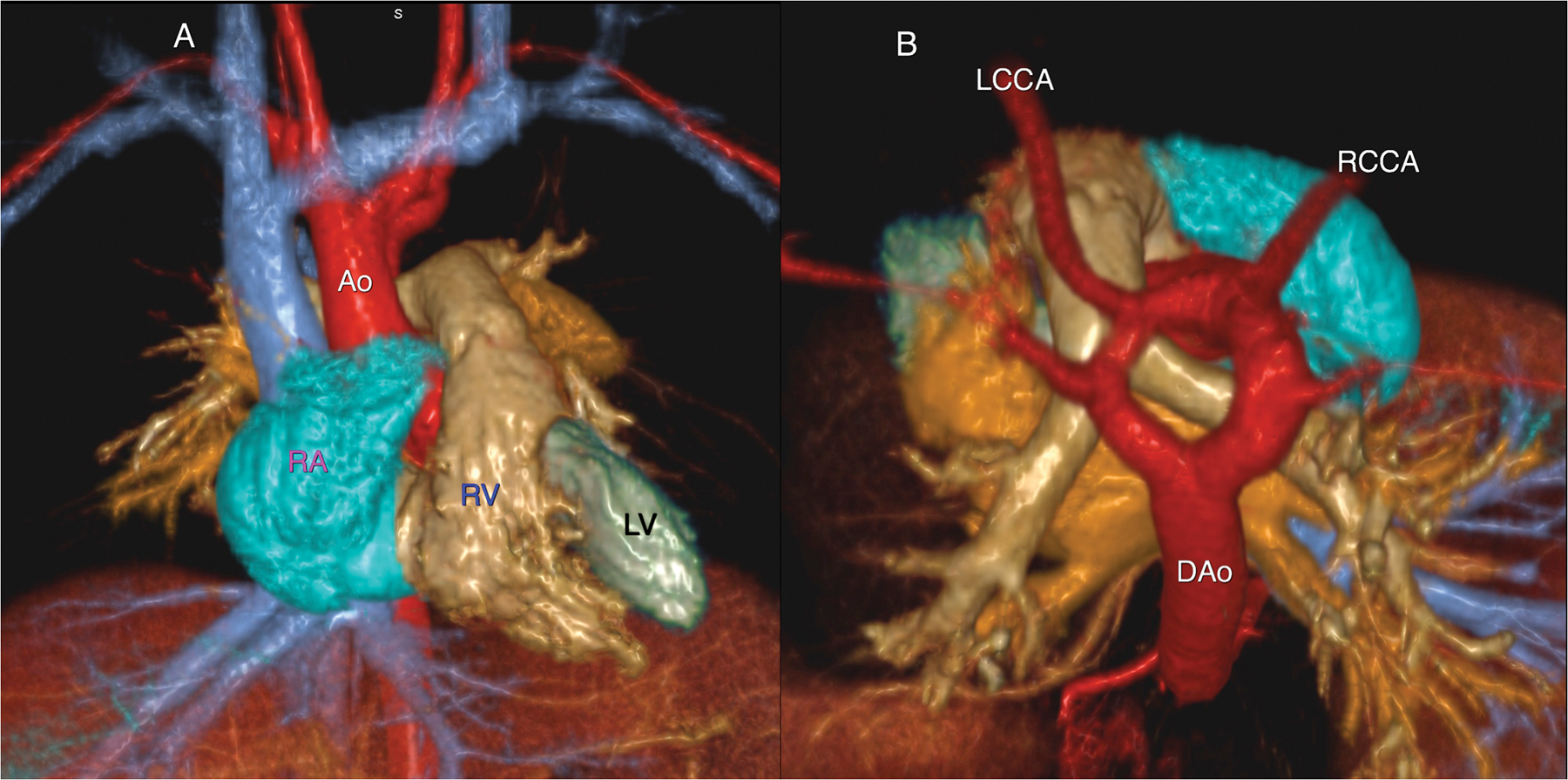
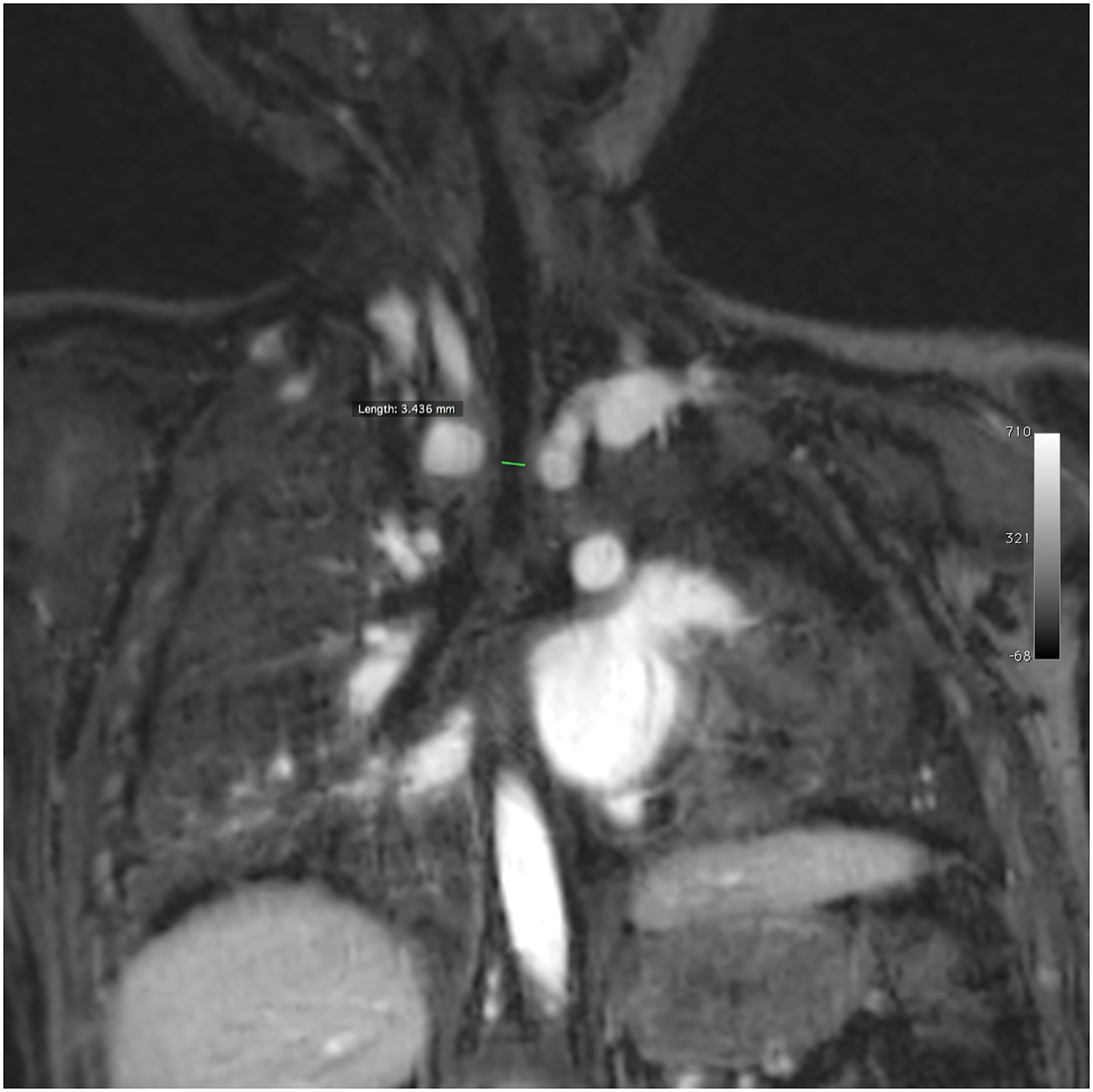
The practice of contrast-enhanced magnetic resonance angiography (CEMRA) has changed significantly in the span of a decade. Concerns regarding gadolinium (Gd)-associated nephrogenic systemic fibrosis in those with severely impaired renal function spurred developments in low-dose CEMRA and non-contrast MRA as well as efforts to seek alternative MR contrast agents. Originally developed for MR imaging use, ferumoxytol (an ultra-small superparamagnetic iron oxide nanoparticle), is currently approved by the US Food and Drug Administration for the treatment of iron deficiency anaemia in adults with renal disease. Since its clinical availability in 2009, there has been rising interest in the scientific and clinical use of ferumoxytol as an MR contrast agent. The unique physicochemical and pharmacokinetic properties of ferumoxytol, including its long intravascular half-life and high r1 relaxivity, support a spectrum of MRI applications beyond the scope of Gd-based contrast agents. Moreover, whereas Gd is not found in biological systems, iron is essential for normal metabolism, and nutritional iron deficiency poses major public health challenges worldwide. Once the carbohydrate shell of ferumoxytol is degraded, the elemental iron at its core is incorporated into the reticuloendothelial system. These considerations position ferumoxytol as a potential game changer in the field of CEMRA and MRI. In this paper, we aim to summarise our experience with the cardiovascular applications of ferumoxytol and provide a brief synopsis of ongoing investigations on ferumoxytol-enhanced MR applications.
Copyright © 2016. Published by Elsevier Ltd.
Figures
Similar articles
-
Emerging applications for ferumoxytol as a contrast agent in MRI.J Magn Reson Imaging. 2015 Apr;41(4):884-98. doi: 10.1002/jmri.24691. Epub 2014 Jun 30. J Magn Reson Imaging. 2015. PMID: 24974785 Review.
-
Ferumoxytol-Enhanced Magnetic Resonance Imaging in Late-Stage CKD.Am J Kidney Dis. 2016 Jun;67(6):984-8. doi: 10.1053/j.ajkd.2015.12.017. Epub 2016 Jan 16. Am J Kidney Dis. 2016. PMID: 26786296 Free PMC article.
-
Relaxivity and In Vivo Human Performance of Brand Name Versus Generic Ferumoxytol.Invest Radiol. 2025 May 1;60(5):319-327. doi: 10.1097/RLI.0000000000001130. Epub 2024 Oct 23. Invest Radiol. 2025. PMID: 39437023
-
Contrast-enhanced magnetic resonance venography in pediatric patients with chronic kidney disease: initial experience with ferumoxytol.Pediatr Radiol. 2016 Aug;46(9):1332-40. doi: 10.1007/s00247-016-3605-z. Epub 2016 Apr 8. Pediatr Radiol. 2016. PMID: 27059620 Free PMC article. Review.
-
Crossover comparison of ferumoxytol and gadobenate dimeglumine for abdominal MR-angiography at 3.0 tesla: Effects of contrast bolus length and flip angle.J Magn Reson Imaging. 2017 Jun;45(6):1617-1626. doi: 10.1002/jmri.25513. Epub 2016 Nov 10. J Magn Reson Imaging. 2017. PMID: 27862577 Free PMC article. Clinical Trial.
Cited by
-
Pathophysiology, classification, and MRI parallels in microvascular disease of the heart and brain.Microcirculation. 2020 Nov;27(8):e12648. doi: 10.1111/micc.12648. Epub 2020 Jul 26. Microcirculation. 2020. PMID: 32640064 Free PMC article. Review.
-
Opportunities in Interventional and Diagnostic Imaging by Using High-Performance Low-Field-Strength MRI.Radiology. 2019 Nov;293(2):384-393. doi: 10.1148/radiol.2019190452. Epub 2019 Oct 1. Radiology. 2019. PMID: 31573398 Free PMC article.
-
Pharmacokinetic Profiling of Unlabeled Magnetic Nanoparticles Using Magnetic Particle Imaging as a Novel Cold Tracer Assay.Nano Lett. 2024 Dec 11;24(49):15557-15564. doi: 10.1021/acs.nanolett.4c03553. Epub 2024 Nov 26. Nano Lett. 2024. PMID: 39591368 Free PMC article.
-
USPIOs as targeted contrast agents in cardiovascular magnetic resonance imaging.Curr Cardiovasc Imaging Rep. 2021 Feb;14(2):2. doi: 10.1007/s12410-021-09552-8. Epub 2021 Feb 26. Curr Cardiovasc Imaging Rep. 2021. PMID: 33824694 Free PMC article.
-
Ferumoxytol-enhanced cardiovascular magnetic resonance detection of early stage acute myocarditis.J Cardiovasc Magn Reson. 2019 Dec 16;21(1):77. doi: 10.1186/s12968-019-0587-7. J Cardiovasc Magn Reson. 2019. PMID: 31842900 Free PMC article.
References
-
- Kuo PH, Kanal E, Abu-Alfa AK, Cowper SE. Gadolinium-based MR contrast agents and nephrogenic systemic fibrosis. Radiology. 2007;242(3):647–649. - PubMed
-
- Deo A, Fogel M, Cowper SE. Nephrogenic systemic fibrosis: a population study examining the relationship of disease development to gadolinium exposure. Clinical journal of the American Society of Nephrology : CJASN. 2007;2(2):264–267. - PubMed
-
- Kanal E, Barkovich AJ, Bell C, et al. ACR guidance document for safe MR practices: 2007. AJR American journal of roentgenology. 2007;188(6):1447–1474. - PubMed
-
- American College of Radiology. ACR Manual on Contrast Media (Version 10). 2015. Accessed September 1, 2015. 79–93. http://www.acr.org/~/media/37D84428BF1D4E1B9A3A2918DA9E27A3.pdf.
-
- Edelman RR, Sheehan JJ, Dunkle E, Schindler N, Carr J, Koktzoglou I. Quiescent-interval single-shot unenhanced magnetic resonance angiography of peripheral vascular disease: Technical considerations and clinical feasibility. Magnetic resonance in medicine : official journal of the Society of Magnetic. 2010;63(4):951–958. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
