

Gametocyte carriage in uncomplicated Plasmodium falciparum malaria following treatment with artemisinin combination therapy: a systematic review and meta-analysis of individual patient data
- PMID: 27221542
- PMCID: PMC4879753
- DOI: 10.1186/s12916-016-0621-7
Gametocyte carriage in uncomplicated Plasmodium falciparum malaria following treatment with artemisinin combination therapy: a systematic review and meta-analysis of individual patient data
Abstract
Background: Gametocytes are responsible for transmission of malaria from human to mosquito. Artemisinin combination therapy (ACT) reduces post-treatment gametocyte carriage, dependent upon host, parasite and pharmacodynamic factors. The gametocytocidal properties of antimalarial drugs are important for malaria elimination efforts. An individual patient clinical data meta-analysis was undertaken to identify the determinants of gametocyte carriage and the comparative effects of four ACTs: artemether-lumefantrine (AL), artesunate/amodiaquine (AS-AQ), artesunate/mefloquine (AS-MQ), and dihydroartemisinin-piperaquine (DP).
Methods: Factors associated with gametocytaemia prior to, and following, ACT treatment were identified in multivariable logistic or Cox regression analysis with random effects. All relevant studies were identified through a systematic review of PubMed. Risk of bias was evaluated based on study design, methodology, and missing data.
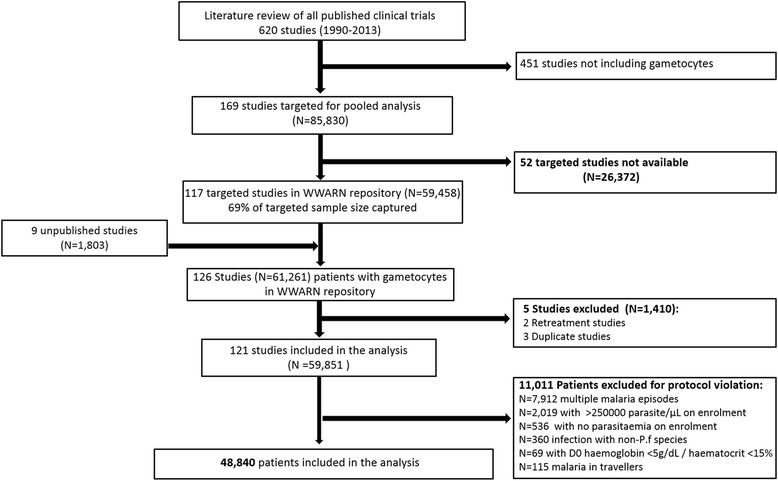
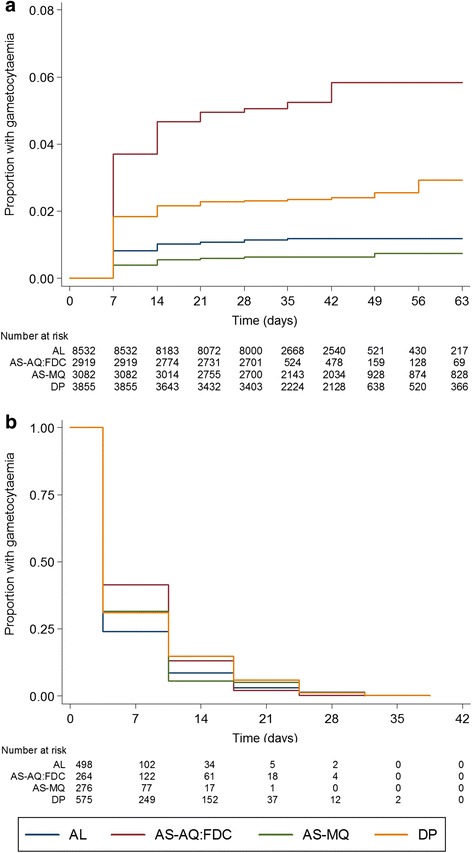
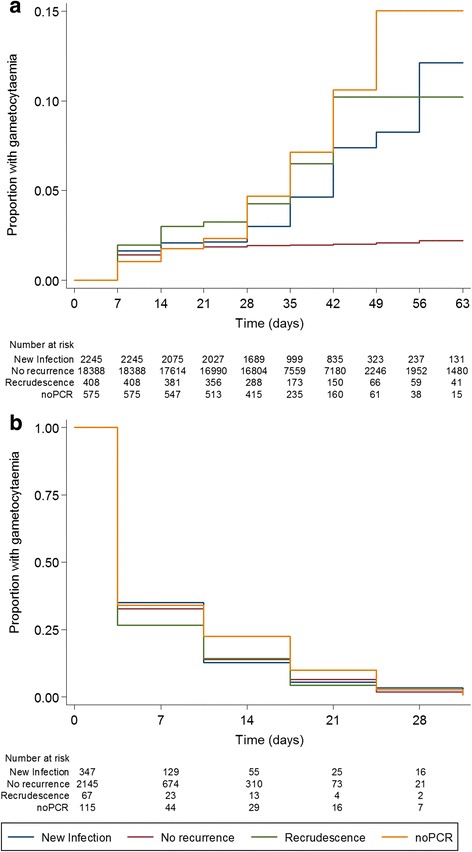
Results: The systematic review identified 169 published and 9 unpublished studies, 126 of which were shared with the WorldWide Antimalarial Resistance Network (WWARN) and 121 trials including 48,840 patients were included in the analysis. Prevalence of gametocytaemia by microscopy at enrolment was 12.1 % (5887/48,589), and increased with decreasing age, decreasing asexual parasite density and decreasing haemoglobin concentration, and was higher in patients without fever at presentation. After ACT treatment, gametocytaemia appeared in 1.9 % (95 % CI, 1.7-2.1) of patients. The appearance of gametocytaemia was lowest after AS-MQ and AL and significantly higher after DP (adjusted hazard ratio (AHR), 2.03; 95 % CI, 1.24-3.12; P = 0.005 compared to AL) and AS-AQ fixed dose combination (FDC) (AHR, 4.01; 95 % CI, 2.40-6.72; P < 0.001 compared to AL). Among individuals who had gametocytaemia before treatment, gametocytaemia clearance was significantly faster with AS-MQ (AHR, 1.26; 95 % CI, 1.00-1.60; P = 0.054) and slower with DP (AHR, 0.74; 95 % CI, 0.63-0.88; P = 0.001) compared to AL. Both recrudescent (adjusted odds ratio (AOR), 9.05; 95 % CI, 3.74-21.90; P < 0.001) and new (AOR, 3.03; 95 % CI, 1.66-5.54; P < 0.001) infections with asexual-stage parasites were strongly associated with development of gametocytaemia after day 7.
Conclusions: AS-MQ and AL are more effective than DP and AS-AQ FDC in preventing gametocytaemia shortly after treatment, suggesting that the non-artemisinin partner drug or the timing of artemisinin dosing are important determinants of post-treatment gametocyte dynamics.
Keywords: Drug resistance; Gametocyte; Malaria; Plasmodium falciparum.
Figures

References
-
- World Health Organization . World Malaria Report 2014. Geneva: WHO; 2014.
-
- Price R, Nosten F, Simpson JA, Luxemburger C, Phaipun L, ter Kuile F, et al. Risk factors for gametocyte carriage in uncomplicated falciparum malaria. Am J Trop Med Hyg. 1999;60(6):1019–23. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
