

Idiopathic granulomatous mastitis: imaging update and review
- PMID: 27221974
- PMCID: PMC4956627
- DOI: 10.1007/s13244-016-0499-0
Idiopathic granulomatous mastitis: imaging update and review
Abstract
Objectives: The purpose of this study was to review the imaging features of idiopathic granulomatous mastitis (IGM) with clinical and pathology correlation.
Methods: With institutional review board (IRB) approval, a retrospective search of the surgical pathology database from January 2000 to July 2015 was performed. Clinical, imaging and histology findings were reviewed. Cases of granulomatous mastitis without a known source, diagnosed with percutaneous or surgical biopsy, were included in our analysis.
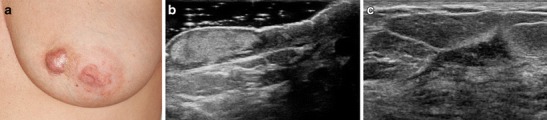
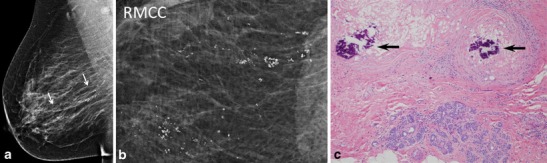
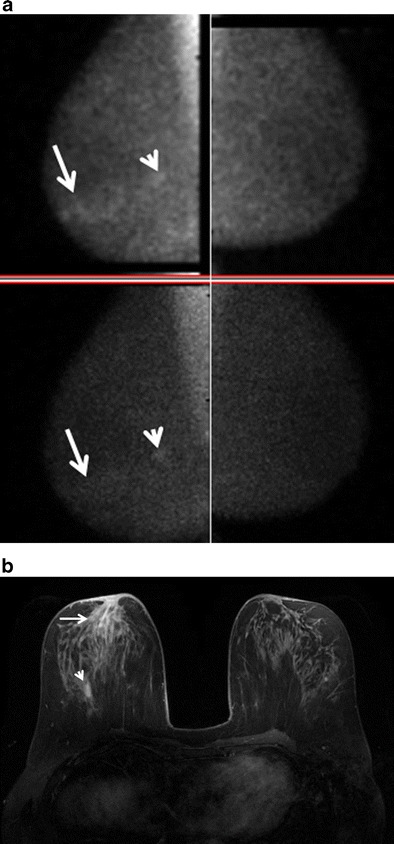
Results: Seventeen cases of IGM were identified with imaging available for review. The majority of patients presented with a palpable abnormality, whereas a minority were asymptomatic with an abnormal screening mammogram. At imaging, IGM most often demonstrated a focal asymmetry at mammography, a hypoechoic mass with irregular or angular margins at ultrasound, and robust enhancement with mixed progressive and plateau kinetics at magnetic resonance imaging (MRI). Axillary lymph nodes were reactive in appearance at ultrasound. Molecular breast imaging performed in one case showed mild focal asymmetric radiotracer uptake.
Conclusion: IGM is a rapidly progressive rare inflammatory condition of the breast resulting in non-necrotizing granuloma formation. Imaging features mimic breast carcinoma and diagnosis can be difficult. Radiologists' awareness of this condition is essential to prevent delayed or unnecessary treatment.
Teaching points: • Idiopathic granulomatous mastitis is rapidly progressive inflammatory condition. • Imaging features may mimic breast carcinoma or infection. • Ultrasound shows irregular hypoechoic masses with increased vascularity and sinus tracts. • MRI shows irregular, enhancing masses or non-mass enhancement with microabscesses. • MRI is useful for assessment of breast involvement and response to treatment.
Keywords: Breast; Breast ultrasound; Granulomatous mastitis; MRI; Mammography.
Figures





References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
