

Clinical Outcomes of Metabolic Surgery: Efficacy of Glycemic Control, Weight Loss, and Remission of Diabetes
- PMID: 27222548
- PMCID: PMC5864131
- DOI: 10.2337/dc16-0382
Clinical Outcomes of Metabolic Surgery: Efficacy of Glycemic Control, Weight Loss, and Remission of Diabetes
Abstract
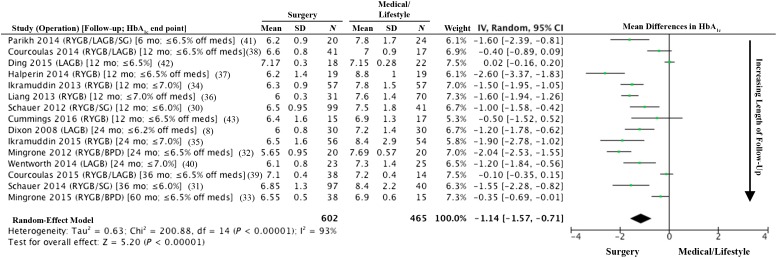
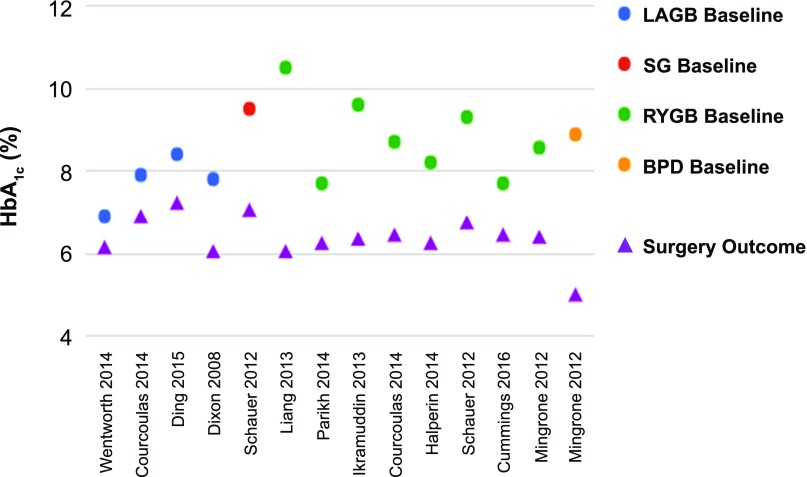
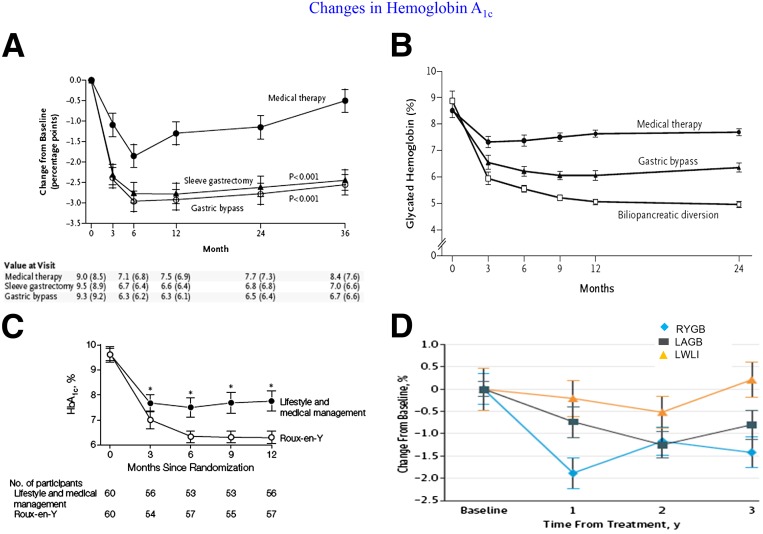
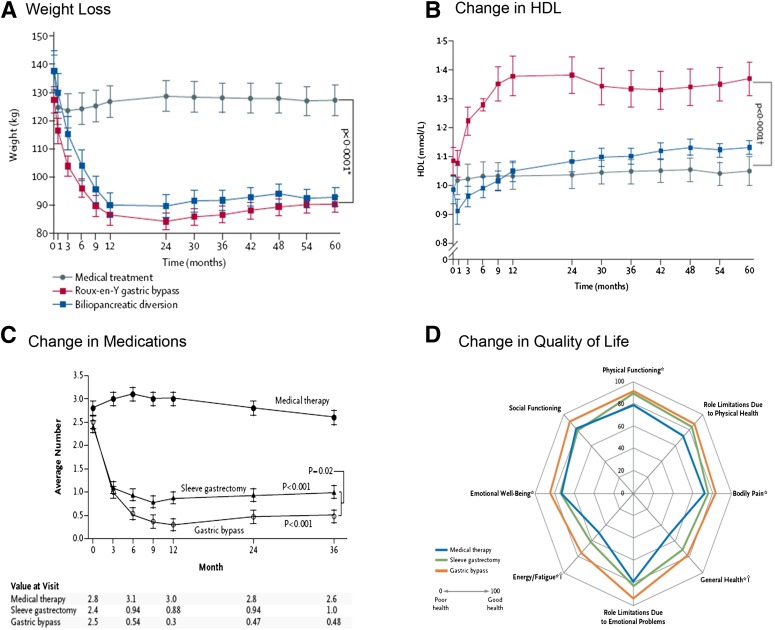
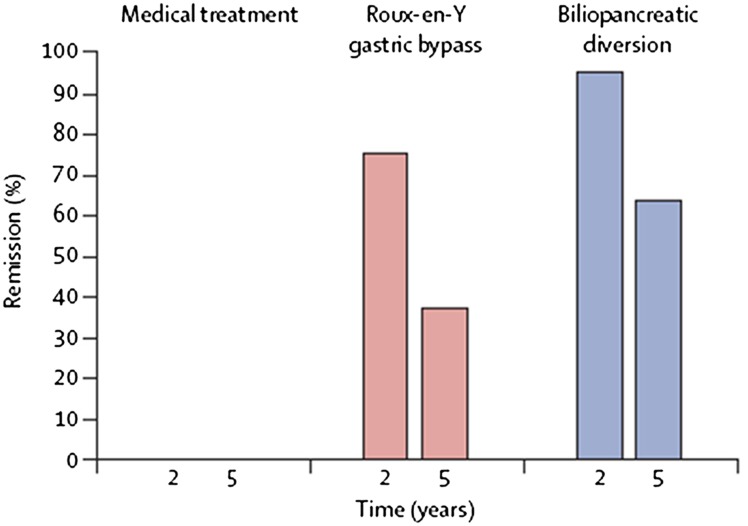
Since the 2007 Diabetes Surgery Summit in Rome, Italy, and the subsequent publishing of the world's first guidelines for the surgical treatment of type 2 diabetes (T2D), much new evidence regarding the efficacy and safety of metabolic surgery has emerged. Additional observational cohort studies support the superior effects of surgery over medical treatment with respect to glycemic control, weight loss, and even reduction in mortality and microvascular complications associated with T2D. Furthermore, new safety data suggest that the perioperative morbidity and mortality of metabolic surgery (5% and 0.3%, respectively) are now similar to that of common low-risk procedures, such as cholecystectomy and hysterectomy. The largest advance, however, has been the completion of 11 randomized controlled trials from around the globe that compare surgery with medical treatment of T2D. These studies with follow-up duration of 1-5 years involve nearly 800 patients without surgical mortality and with major complication rates of less than 5% and a reoperation rate of 8%. All but 1 of the 11 randomized controlled trials have shown the superiority of surgery over medical management at achieving remission or glycemic improvement. Surgery was also superior to medical treatment with respect to improving cardiovascular risk factors, such as weight loss and dyslipidemia, while reducing medication burden. This new efficacy and safety evidence should help guide physicians across the globe to the appropriate use of surgery as an effective treatment for patients suffering from T2D and obesity.
© 2016 by the American Diabetes Association. Readers may use this article as long as the work is properly cited, the use is educational and not for profit, and the work is not altered.
Figures
References
-
- Holst JJ, Gribble F, Horowitz M, Rayner CK. Roles of the gut in glucose homeostasis. Diabetes Care 2016;39:884–892 - PubMed
-
- Angrisani L, Santonicola A, Iovino P, Formisano G, Buchwald H, Scopinaro N. Bariatric surgery worldwide 2013. Obes Surg 2015;25:1822–1832 - PubMed
-
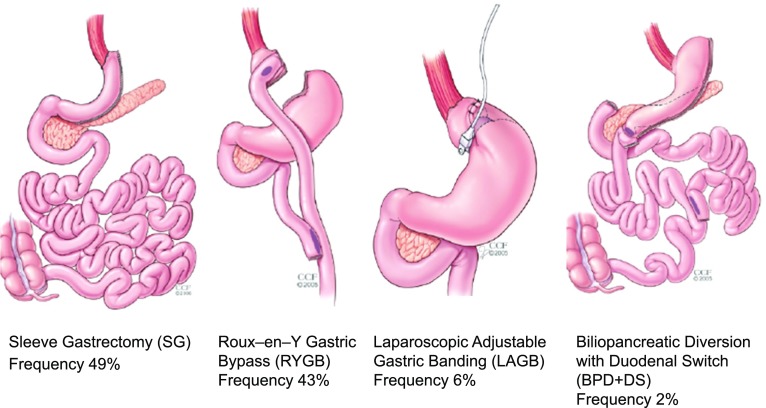
- Khorgami Z, Andalib A, Corcelles R, Aminian A, Brethauer S, Schauer P. Recent national trends in the surgical treatment of obesity: sleeve gastrectomy dominates. Surg Obes Relat Dis 2015;11:S6–S8
-
- Consensus Development Conference Panel NIH conference. Gastrointestinal surgery for severe obesity. Ann Intern Med 1991;115:956–961 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
