

Clinical features and outcome of bone and joint infections with streptococcal involvement: 5-year experience of interregional reference centres in the south of France
- PMID: 27222712
- PMCID: PMC4872313
- DOI: 10.1016/j.nmni.2016.03.009
Clinical features and outcome of bone and joint infections with streptococcal involvement: 5-year experience of interregional reference centres in the south of France
Abstract
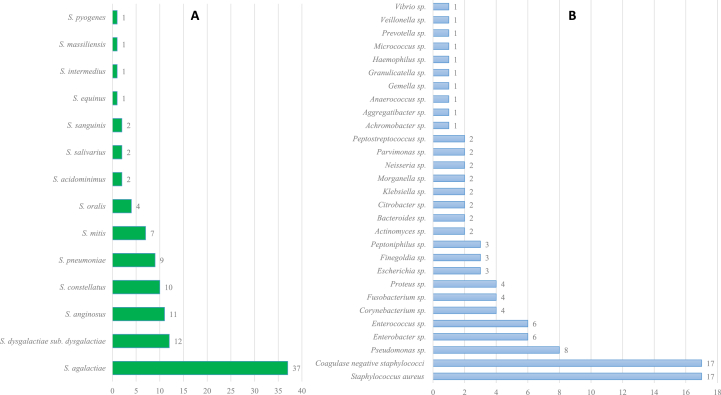
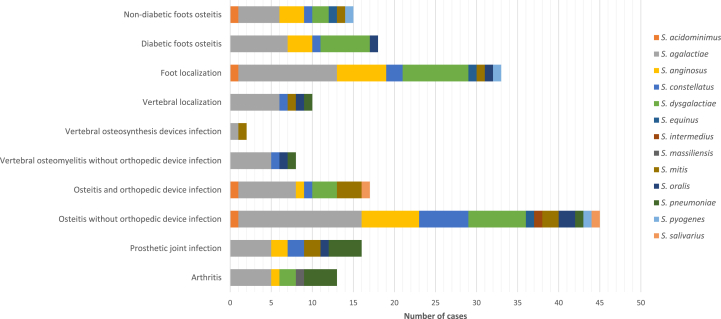
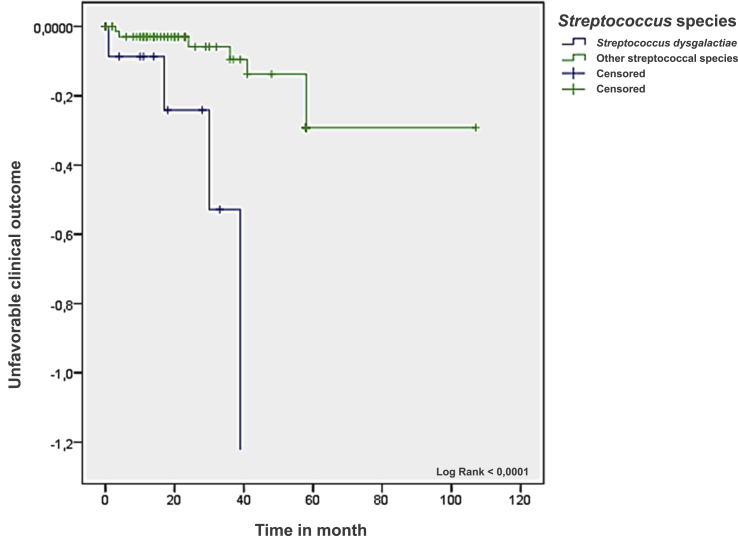
Streptococcal bone and joint infections are less common than staphylococcal cases. Few studies have reported the cases with well-identified Streptococcus species. Their clinical features and prognosis are not clearly known to date. Moreover, no treatment regimen has yet been clarified. We reviewed the streptococcal bone and joint infection cases managed in our centres from January 2009 to December 2013. We described the epidemiology, clinical and microbiologic characteristics, treatment approach and outcome. Among the 93 cases, 83% of patients were men with a median age of 60 years, and 90% of patients had comorbidities or risk factors. Bacteraemia occurred in 14% of cases. Serious complications occurred in six patients, including severe sepsis (two cases) and infective endocarditis (two cases). Orthopaedic device infections were observed in 35% of cases, including 17 patients with internal osteosynthesis device infection, 14 with prosthetic joint infection and three with vertebral osteosynthesis device infection. The median time between orthopaedic device implantation and onset of infection was 447 days. Fourteen species of Streptococcus were identified, including 97 isolates using matrix-assisted laser desorption/ionization time-of-flight mass spectrometry and three isolates using molecular identification. The five most represented species included S. agalactiae (37%), S. dysgalactiae (12%), S. anginosus (11%), S. constellatus (10%) and S. pneumoniae (9%). Streptococci isolates were susceptible to amoxicillin, with the exception of one S. mitis isolate. Remission 1 year after the end of treatment was recorded in 83%. One patient died of infection; eight patients had infections that failed to respond to treatment; and seven patients experienced relapse. Twenty patients (22%) had an unfavourable functional outcome, including 19 amputations and one arthrodesis. Five significant prognostic factors associated with an unfavourable clinical outcome were identified, including peripheral neuropathy (p 0.009), peripheral arterial disease (p 0.019), diabetes mellitus (p 0.031), location in the femur (p 0.0036), location in the foot (p 0.0475), osteitis without an orthopaedic device (p 0.041) and infection caused by S. dysgalactiae (p 0.020). The rate of poor outcomes remains high despite the low number of Streptococcus isolates resistant to antibiotics. Some prognostic factors, such as the presence of S. dysgalactiae, are associated with an unfavourable clinical outcome. Antibiotic regimens of streptococcal bone and joint infections are not standardized and need to be further investigated.
Keywords: Arthritis; MALDI-TOF MS; Streptococcus; bacterial infection; bone and joint infection; human; osteitis; osteomyelitis; prosthetic joint infection; streptococci.
Figures
References
-
- Lipsky B.A., Weigelt J.A., Gupta V., Killian A., Peng M.M. Skin, soft tissue, bone, and joint infections in hospitalized patients: epidemiology and microbiological, clinical, and economic outcomes. Infect Control Hosp Epidemiol. 2007;28:1290–1298. - PubMed
-
- Phillips J.E., Crane T.P., Noy M., Elliott T.S.J., Grimer R.J. The incidence of deep prosthetic infections in a specialist orthopaedic hospital: a 15-year prospective survey. J Bone Joint Surg Br. 2006;88:943–948. - PubMed
-
- Ryan M.J., Kavanagh R., Wall P.G., Hazleman B.L. Bacterial joint infections in England and Wales: analysis of bacterial isolates over a four year period. Br J Rheumatol. 1997;36:370–373. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources