

Emerging immunotherapies for glioblastoma
- PMID: 27223671
- PMCID: PMC4915370
- DOI: 10.1080/14728214.2016.1186643
Emerging immunotherapies for glioblastoma
Abstract
Introduction: Immunotherapy for brain cancer has evolved dramatically over the past decade, owed in part to our improved understanding of how the immune system interacts with tumors residing within the central nervous system (CNS). Glioblastoma (GBM), the most common primary malignant brain tumor in adults, carries a poor prognosis (<15 months) and only few advances have been made since the FDA's approval of temozolomide (TMZ) in 2005. Importantly, several immunotherapies have now entered patient trials based on promising preclinical data, and recent studies have shed light on how GBM employs a slew of immunosuppressive mechanisms that may be targeted for therapeutic gain. Altogether, accumulating evidence suggests immunotherapy may soon earn its keep as a mainstay of clinical management for GBM.
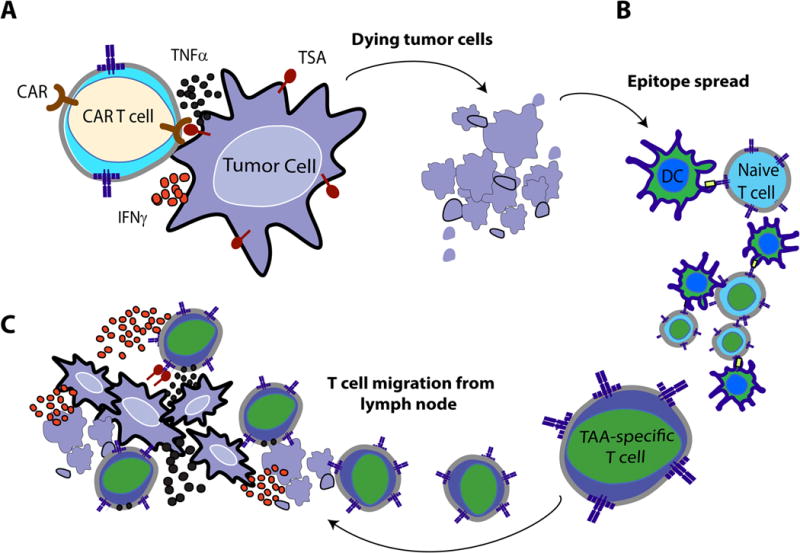
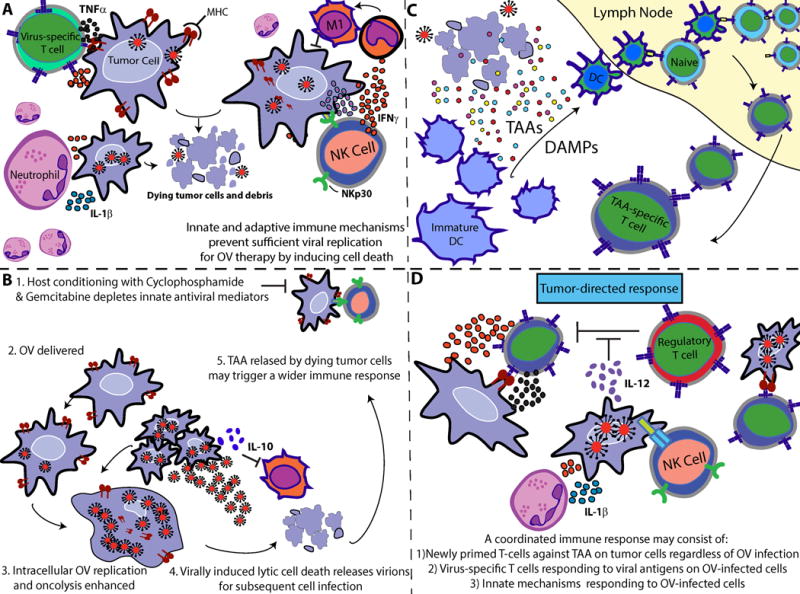
Areas covered: Here, we review cancer vaccines, checkpoint inhibitors, adoptive T-cell immunotherapy, and oncolytic virotherapy.
Expert opinion: Checkpoint blockade induces antitumor activity by preventing negative regulation of T-cell activation. This platform, however, depends on an existing frequency of tumor-reactive T cells. GBM tumors are exceptionally equipped to prevent this, occupying low levels of antigen expression and elaborate mechanisms of immunosuppression. Therefore, checkpoint blockade may be most effective when used in combination with a DC vaccine or adoptively transferred tumor-specific T cells generated ex vivo. Both approaches have been shown to induce endogenous immune responses against tumor antigens, providing a rationale for use with checkpoint blockade where both primary and secondary responses may be potentiated.
Keywords: CDX-110; EGFRvIII; GBM; checkpoint inhibitor; chimeric antigen receptor t cells; dendritic cell vaccine; glioblastoma; glioblastoma multiforme; immune system; immunotherapy; ipilimumab; monoclonal antibody; nivolumab; oncolytic virus; peptide vaccine; rindopepimut; tumor lysate vaccine.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous