

Varicella zoster virus triggers the immunopathology of giant cell arteritis
- PMID: 27224742
- PMCID: PMC4896311
- DOI: 10.1097/BOR.0000000000000292
Varicella zoster virus triggers the immunopathology of giant cell arteritis
Abstract
Purpose of review: Giant cell arteritis (GCA) is a severe form of vasculitis in the elderly. The recent discovery of varicella zoster virus (VZV) in the temporal arteries and adjacent skeletal muscle of patients with GCA, and the rationale and strategy for antiviral and corticosteroid treatment for GCA are reviewed.
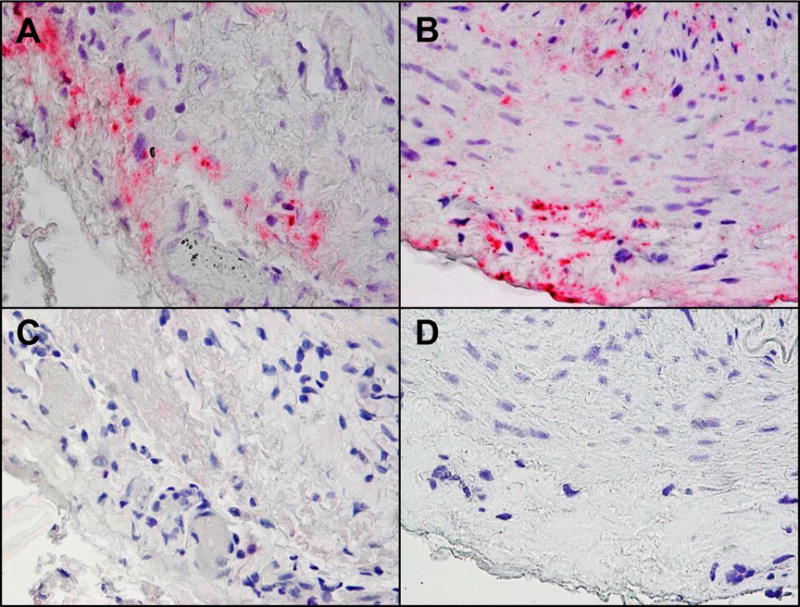
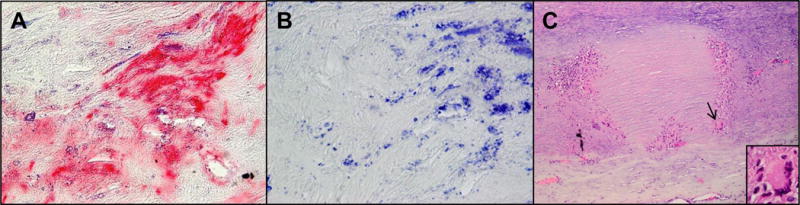
Recent findings: The clinical features of GCA include excruciating headache/head pain, often with scalp tenderness, a nodular temporal arteries and decreased temporal artery pulsations. Jaw claudication, night sweats, fever, malaise, and a history of polymyalgia rheumatica (aching and stiffness of large muscles primarily in the shoulder girdle, upper back, and pelvis without objective signs of weakness) are common. ESR and CRP are usually elevated. Diagnosis is confirmed by temporal artery biopsy which reveals vessel wall damage and inflammation, with multinucleated giant cells and/or epithelioid macrophages. Skip lesions are common. Importantly, temporal artery biopsies are pathologically negative in many clinically suspect cases. This review highlights recent virological findings in temporal arteries from patients with pathologically verified GCA and in temporal arteries from patients who manifest clinical and laboratory features of GCA, but whose temporal artery biopsies (Bx) are pathologically negative for GCA (Bx-negative GCA). Virological analysis revealed that VZV is present in most GCA-positive and GCA-negative temporal artery biopsies, mostly in skip areas that correlate with adjacent GCA pathology.
Summary: The presence of VZV in Bx-positive and Bx-negative GCA temporal arteries indicates that VZV triggers the immunopathology of GCA. However, the presence of VZV in about 20% of temporal artery biopsies from non-GCA postmortem controls also suggests that VZV alone is not sufficient to produce disease. Treatment trials should be performed to determine if antiviral agents confer additional benefits to corticosteroids in both Bx-positive and Bx-negative GCA patients. These studies should also examine whether oral antiviral agents and corticosteroids are as effective as intravenous acyclovir and corticosteroids. Appropriate dosage and duration of treatment also remain to be determined.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Varicella zoster virus and giant cell arteritis.Curr Opin Infect Dis. 2016 Jun;29(3):275-9. doi: 10.1097/QCO.0000000000000258. Curr Opin Infect Dis. 2016. PMID: 26871403 Free PMC article. Review.
-
Analysis of Varicella-Zoster Virus in Temporal Arteries Biopsy Positive and Negative for Giant Cell Arteritis.JAMA Neurol. 2015 Nov;72(11):1281-7. doi: 10.1001/jamaneurol.2015.2101. JAMA Neurol. 2015. PMID: 26349037 Free PMC article.
-
Varicella zoster virus in the temporal artery of a patient with giant cell arteritis.J Neurol Sci. 2013 Dec 15;335(1-2):228-30. doi: 10.1016/j.jns.2013.09.034. Epub 2013 Oct 2. J Neurol Sci. 2013. PMID: 24125020 Free PMC article.
-
Blinded search for varicella zoster virus in giant cell arteritis (GCA)-positive and GCA-negative temporal arteries.J Neurol Sci. 2016 May 15;364:141-3. doi: 10.1016/j.jns.2016.03.020. Epub 2016 Mar 19. J Neurol Sci. 2016. PMID: 27084233 Free PMC article.
-
Developments in Varicella Zoster Virus Vasculopathy.Curr Neurol Neurosci Rep. 2016 Feb;16(2):12. doi: 10.1007/s11910-015-0614-5. Curr Neurol Neurosci Rep. 2016. PMID: 26750127 Free PMC article. Review.
Cited by
-
Pro-inflammatory and anti-inflammatory T cells in giant cell arteritis.Joint Bone Spine. 2017 Jul;84(4):421-426. doi: 10.1016/j.jbspin.2016.07.005. Epub 2016 Sep 20. Joint Bone Spine. 2017. PMID: 27663755 Free PMC article. Review.
-
The Treatment of Giant Cell Arteritis.Curr Treat Options Neurol. 2017 Jan;19(1):2. doi: 10.1007/s11940-017-0440-y. Curr Treat Options Neurol. 2017. PMID: 28138903 Review.
-
Review: What Is the Current Evidence for Disease Subsets in Giant Cell Arteritis?Arthritis Rheumatol. 2018 Sep;70(9):1366-1376. doi: 10.1002/art.40520. Epub 2018 Jul 30. Arthritis Rheumatol. 2018. PMID: 29648680 Free PMC article. Review.
-
Updates in the Diagnosis and Management of Giant Cell Arteritis.Curr Neurol Neurosci Rep. 2019 Aug 8;19(9):68. doi: 10.1007/s11910-019-0982-3. Curr Neurol Neurosci Rep. 2019. PMID: 31396718 Review.
-
Cell Intrinsic Determinants of Alpha Herpesvirus Latency and Pathogenesis in the Nervous System.Viruses. 2023 Nov 22;15(12):2284. doi: 10.3390/v15122284. Viruses. 2023. PMID: 38140525 Free PMC article. Review.
References
-
- Gilden DH, Kleinschmidt-DeMasters BK, Wellish BS, et al. Varicella zoster virus, a cause of waxing and waning vasculitis: The New England Journal of Medicine case 5-1995 revisited. Neurology. 1996;47:1441–1446. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
