

Hemodynamic Stability to Surface Warming and Cooling During Sustained and Continuous Simulated Hemorrhage in Humans
- PMID: 27224744
- PMCID: PMC4976053
- DOI: 10.1097/SHK.0000000000000661
Hemodynamic Stability to Surface Warming and Cooling During Sustained and Continuous Simulated Hemorrhage in Humans
Abstract
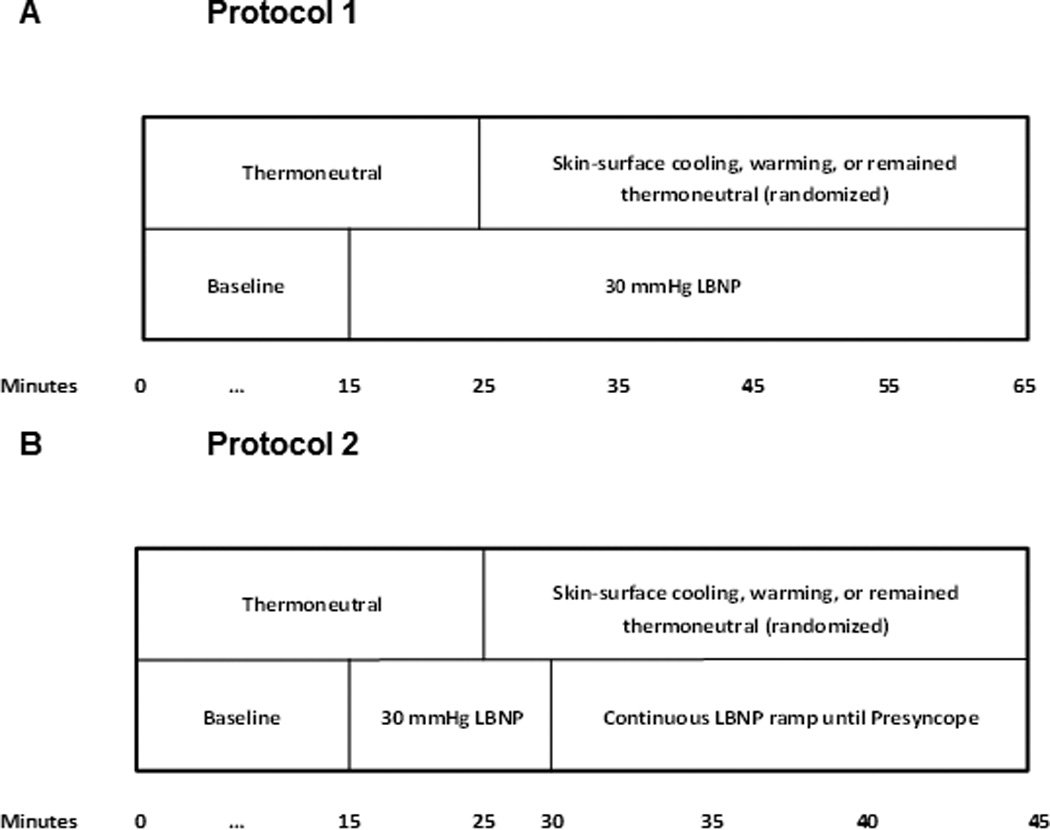
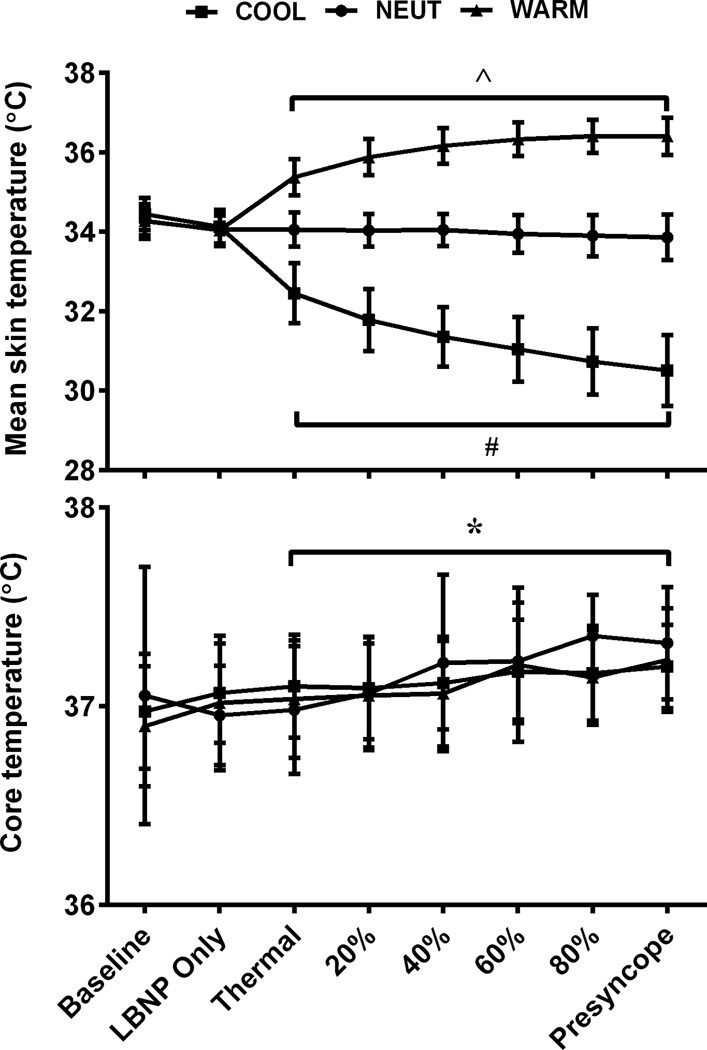
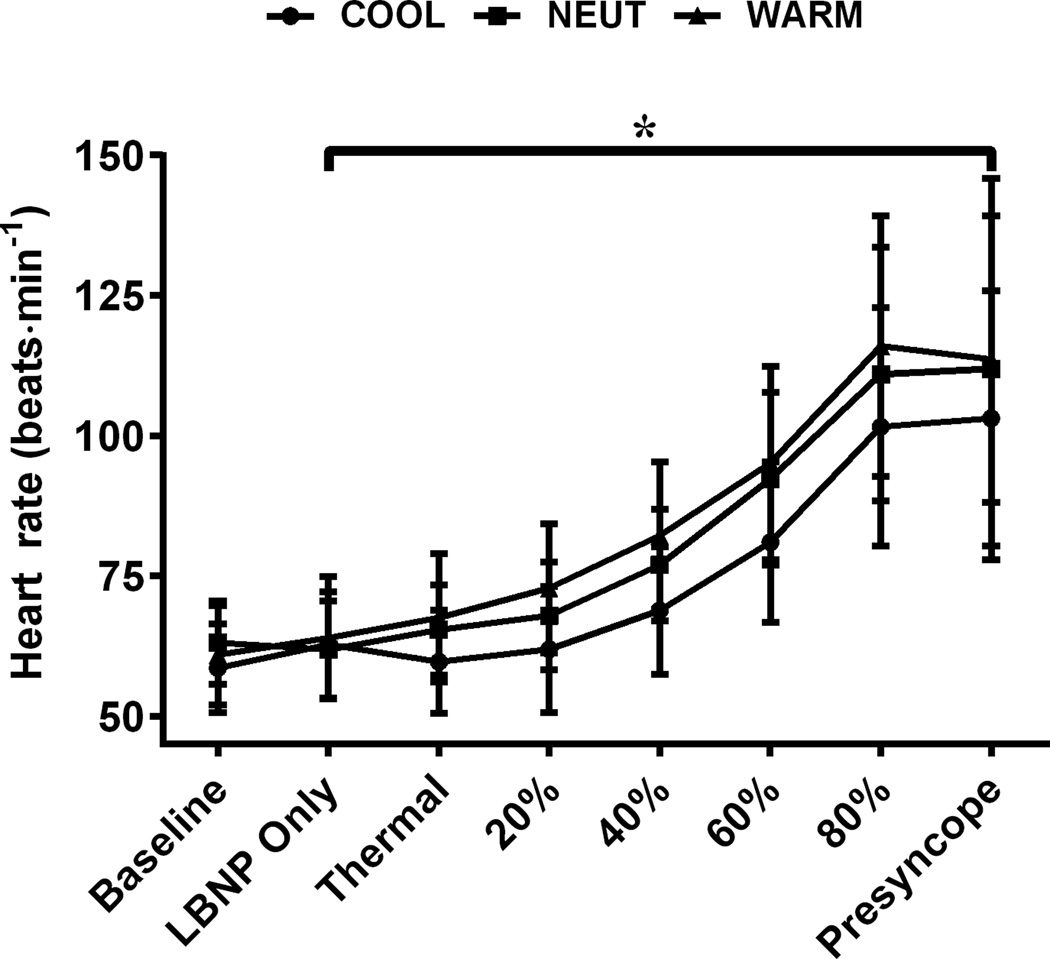
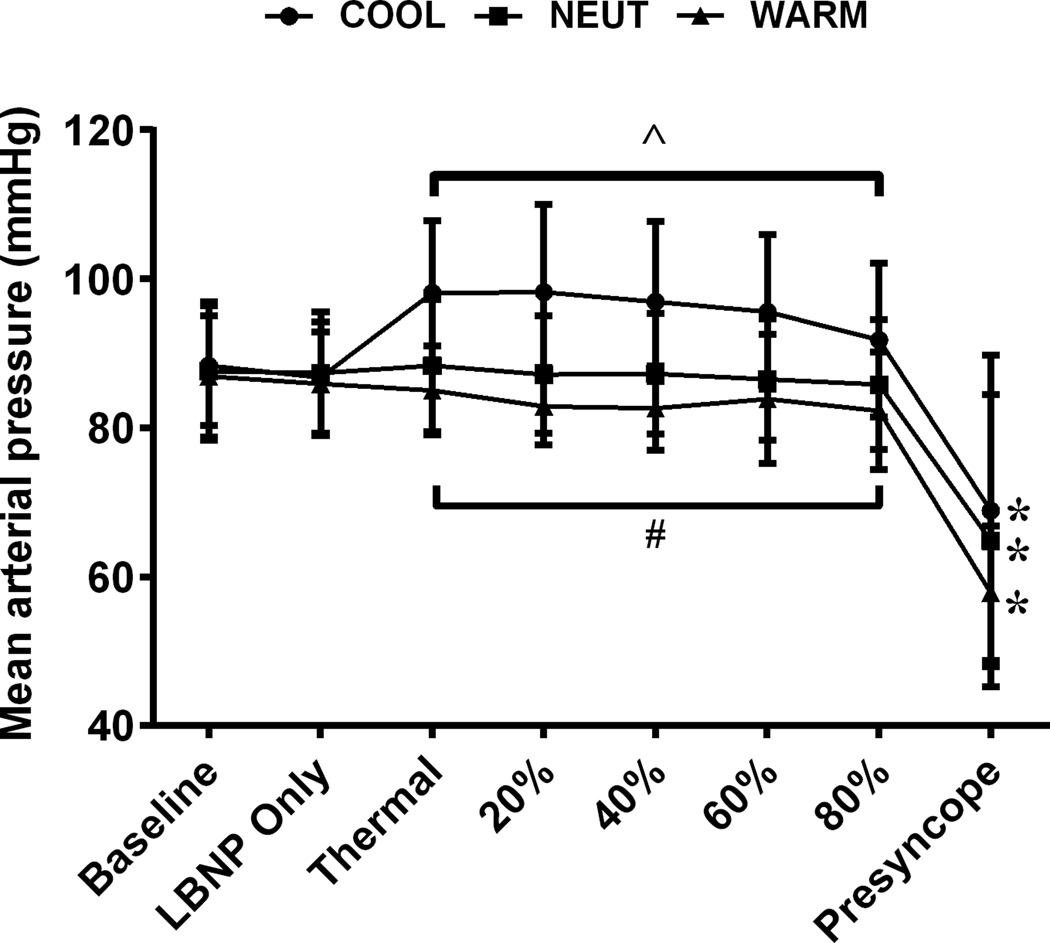
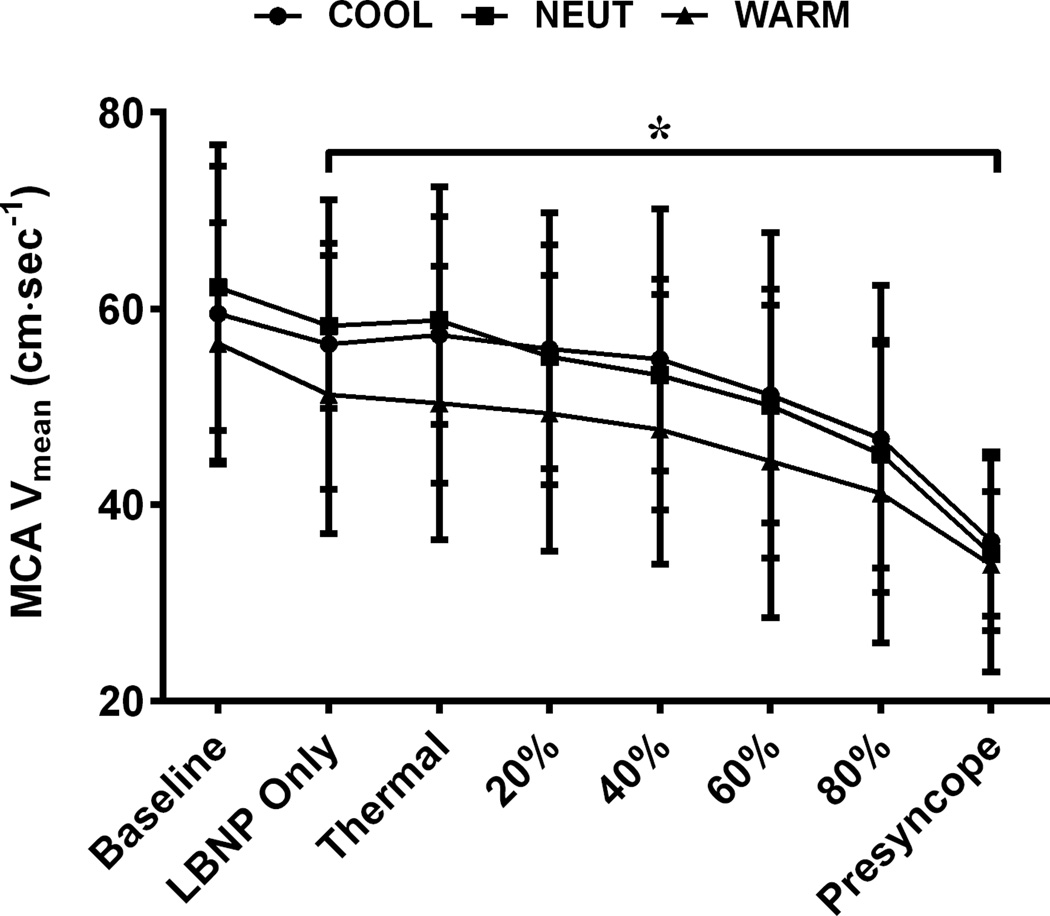
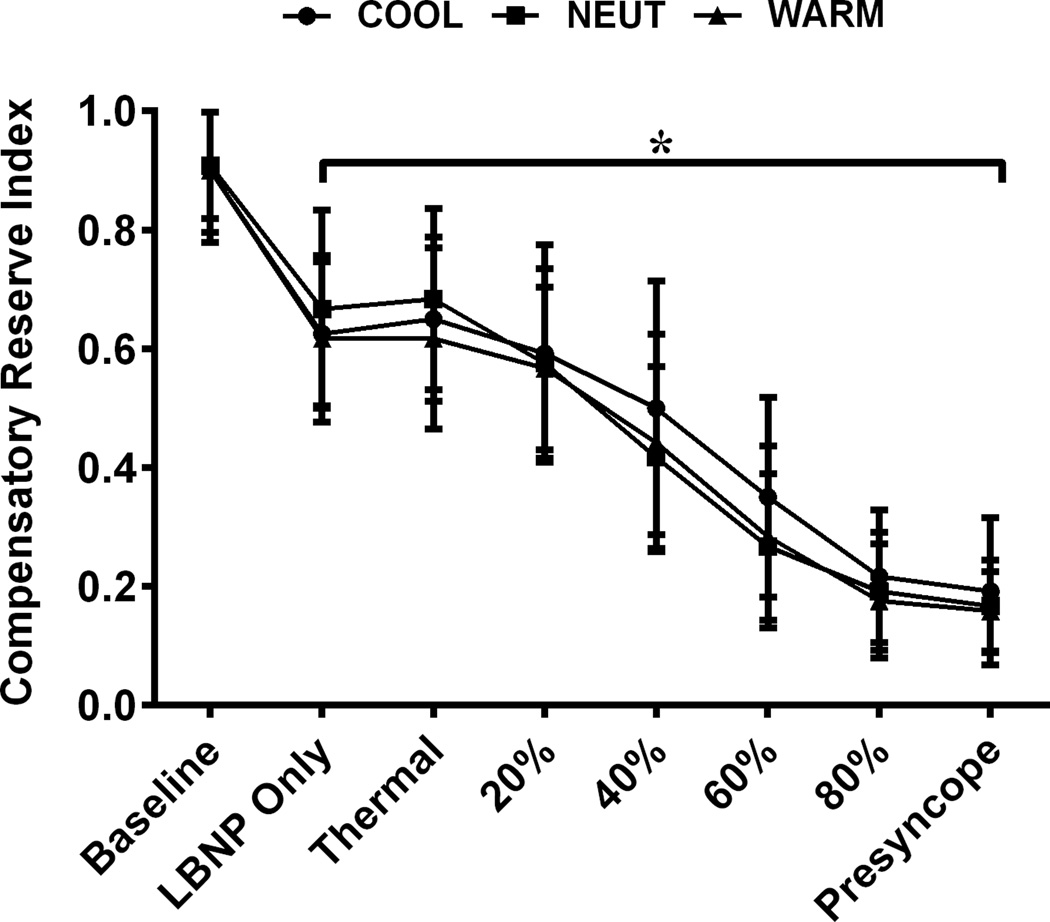
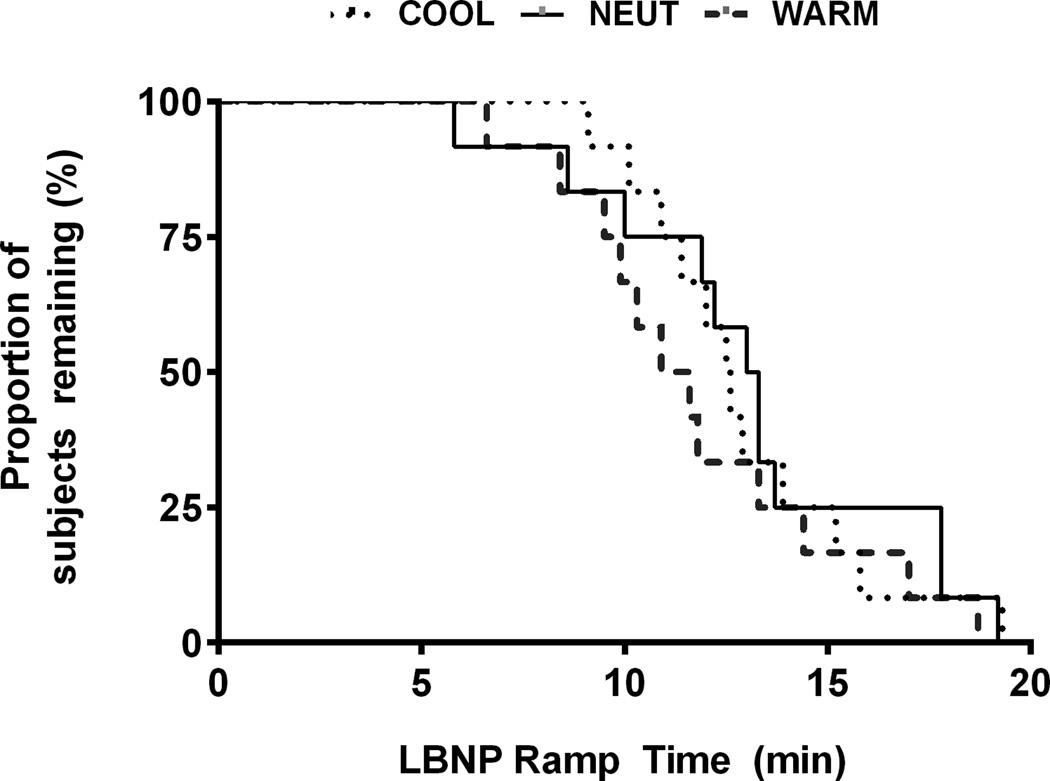
One in 10 deaths worldwide is caused by traumatic injury, and 30% to 40% of those trauma-related deaths are due to hemorrhage. Currently, warming a bleeding victim is the standard of care due to the adverse effects of combined hemorrhage and hypothermia on survival. We tested the hypothesis that heating is detrimental to the maintenance of arterial pressure and cerebral perfusion during hemorrhage, while cooling is beneficial to victims who are otherwise normothermic. Twenty-one men (31 ± 9 y) were examined under two separate protocols designed to produce central hypovolemia similar to hemorrhage. Following 15 min of supine rest, 10 min of 30 mm Hg of lower body negative pressure (LBNP) was applied. On separate randomized days, subjects were then exposed to skin surface cooling (COOL), warming (WARM), or remained thermoneutral (NEUT), while LBNP continued. Subjects remained in these thermal conditions for either 40 min of 30 mm Hg LBNP (N = 9), or underwent a continuous LBNP ramp until hemodynamic decompensation (N = 12). Arterial blood pressure during LBNP was dependent on the thermal perturbation as blood pressure was greater during COOL (P >0.001) relative to NEUT and WARM for both protocols. Middle cerebral artery blood velocity decreased (P <0.001) from baseline throughout sustained and continuous LBNP, but the magnitude of reduction did not differ between thermal conditions. Contrary to our hypothesis, WARM did not reduce cerebral blood velocity or LBNP tolerance relative to COOL and NEUT in normothermic individuals. While COOL increased blood pressure, cerebral perfusion and time to presyncope were not different relative to NEUT or WARM during sustained or continuous LBNP. Warming an otherwise normothermic hemorrhaging victim is not detrimental to hemodynamic stability, nor is this stability improved with cooling.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the author(s).
Figures
Similar articles
-
A comparison of protocols for simulating hemorrhage in humans: step versus ramp lower body negative pressure.J Appl Physiol (1985). 2021 Feb 1;130(2):380-389. doi: 10.1152/japplphysiol.00230.2020. Epub 2020 Nov 19. J Appl Physiol (1985). 2021. PMID: 33211600 Free PMC article.
-
Skin heating during simulated hemorrhage lowers arterial blood pressure but not tolerance following exercise in a cold environment.J Appl Physiol (1985). 2024 Nov 1;137(5):1313-1323. doi: 10.1152/japplphysiol.00560.2024. Epub 2024 Sep 19. J Appl Physiol (1985). 2024. PMID: 39298617
-
Cerebral blood velocity regulation during progressive blood loss compared with lower body negative pressure in humans.J Appl Physiol (1985). 2015 Sep 15;119(6):677-85. doi: 10.1152/japplphysiol.00127.2015. Epub 2015 Jul 2. J Appl Physiol (1985). 2015. PMID: 26139213 Free PMC article.
-
Lower Body Negative Pressure: Physiological Effects, Applications, and Implementation.Physiol Rev. 2019 Jan 1;99(1):807-851. doi: 10.1152/physrev.00006.2018. Physiol Rev. 2019. PMID: 30540225 Review.
-
The reciprocal relationship between cardiac baroreceptor sensitivity and cerebral autoregulation during simulated hemorrhage in humans.Auton Neurosci. 2022 Sep;241:103007. doi: 10.1016/j.autneu.2022.103007. Epub 2022 Jun 11. Auton Neurosci. 2022. PMID: 35716525 Free PMC article. Review.
Cited by
-
A comparison of protocols for simulating hemorrhage in humans: step versus ramp lower body negative pressure.J Appl Physiol (1985). 2021 Feb 1;130(2):380-389. doi: 10.1152/japplphysiol.00230.2020. Epub 2020 Nov 19. J Appl Physiol (1985). 2021. PMID: 33211600 Free PMC article.
References
-
- Hoyt DB, Dutton RP, Hauser CJ, Hess JR, Holcomb JB, Kluger Y, Mackway-Jones K, Parr MJ, Rizoli SB, Yukioka T, Bouillon B. Management of coagulopathy in patients with multiple injuries: Results from an international survey of clinical practice. J Trauma. 2008;65:755–765. - PubMed
-
- Eastridge BJ, Cantrell J, Oetjen-Gerdes L, Zubko T, Mallak C, Wade CE, Simmons J, Mace J, Mabry R, Bolenbaucher R, Blackbourne LH. Died of wounds on the battlefield: Causation and implications for improving combat casualty care. J Trauma. 2011;71:S4–S8. - PubMed
-
- Heckbert SR, Vedder NB, Hoffman W, Winn RK, Hudson LD, Jurkovich GJ, Copass MK, Harlan JM, Rice CL, Maier RV. Outcome after hemorrhagic shock in trauma patients. J Trauma. 1998;45:545–549. - PubMed
-
- Novak V, Novak P, Spies JM, Low PA. Autoregulation of cerebral blood flow in orthostatic hypotension. Stroke. 1998;29:104–111. - PubMed
-
- Tzeng YC, Ainslie PN, Cooke WH, Peeble KC, Willie CK, MacRae BA, Smirl JD, Horsman HM, Rickards CA. Assessment of cerebral autoregulation: The quandary of quantification. Am J Physiol Heart Circ Physiol. 2012;303:H658–H671. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
