

Effectiveness of a hospital-initiated smoking cessation programme: 2-year health and healthcare outcomes
- PMID: 27225016
- PMCID: PMC5543264
- DOI: 10.1136/tobaccocontrol-2015-052728
Effectiveness of a hospital-initiated smoking cessation programme: 2-year health and healthcare outcomes
Abstract
Background: Tobacco-related illnesses are leading causes of death and healthcare use. Our objective was to determine whether implementation of a hospital-initiated smoking cessation intervention would reduce mortality and downstream healthcare usage.
Methods: A 2-group effectiveness study was completed comparing patients who received the 'Ottawa Model' for Smoking Cessation intervention (n=726) to usual care controls (n=641). Participants were current smokers, >17 years old, and recruited during admission to 1 of 14 participating hospitals in Ontario, Canada. Baseline data were linked to healthcare administrative data. Competing-risks regression analysis was used to compare outcomes between groups.
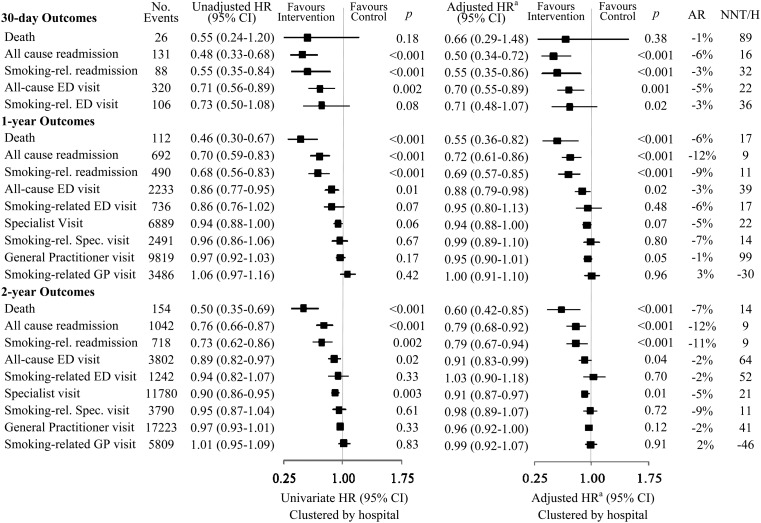
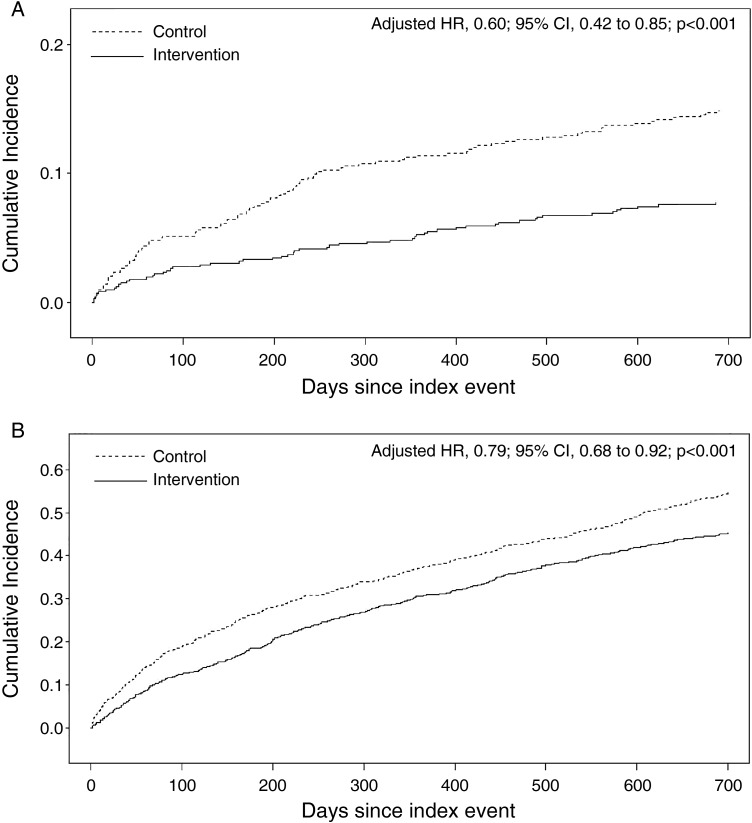
Results: The intervention group experienced significantly lower rates of all-cause readmissions, smoking-related readmissions, and all-cause emergency department (ED) visits at all time points. The largest absolute risk reductions (ARR) were observed for all-cause readmissions at 30 days (13.3% vs 7.1%; ARR, 6.1% (2.9% to 9.3%); p<0.001), 1 year (38.4% vs 26.7%; ARR, 11.7% (6.7% to 16.6%); p<0.001), and 2 years (45.2% vs 33.6%; ARR, 11.6% (6.5% to 16.8%); p<0.001). The greatest reduction in risk of all-cause ED visits was at 30 days (20.9% vs 16.4%; ARR, 4.5% (0.4% to 8.7%); p=0.03). Reduction in mortality was not evident at 30 days, but significant reductions were observed by year 1 (11.4% vs 5.4%; ARR 6.0% (3.1% to 9.0%); p<0.001) and year 2 (15.1% vs 7.9%; ARR, 7.3% (3.9% to 10.7%); p<0.001).
Conclusions: Considering the relatively low cost, greater adoption of hospital-initiated tobacco cessation interventions should be considered to improve patient outcomes and decrease subsequent healthcare usage.
Keywords: Cessation; Health Services; Priority/special populations.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
Figures
References
-
- World Health Organization. WHO Report on the global tobacco epidemic, 2013: Enforcing bans on tobacco advertising, promotion and sponsorship. Geneva: 2013. http://www.who.int/tobacco/global_report/2013/en/ (accessed Aug 2014).
-
- The Health Consequences of Smoking: 50 Years of Progress. A Report of the Surgeon General. Atlanta: Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2014. http://www.surgeongeneral.gov/library/reports/50-years-of-progress/front... (accessed 12 Jul 2014).
-
- Fiore MC, Jaen CR, Baker TB, et al. . Treating tobacco use and dependence: 2008 update. Rockville, MD, USA: Department of Health and Human Services, 2008:12.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical