

The dosimetric impact of implants on the spinal cord dose during stereotactic body radiotherapy
- PMID: 27225270
- PMCID: PMC4880816
- DOI: 10.1186/s13014-016-0649-z
The dosimetric impact of implants on the spinal cord dose during stereotactic body radiotherapy
Abstract
Background: The effects of spinal implants on dose distribution have been studied for conformal treatment plans. However, the dosimetric impact of spinal implants in stereotactic body radiotherapy (SBRT) treatments has not been studied in spatial orientation. In this study we evaluated the effect of spinal implants placed in sawbone vertebra models implanted as in vivo instrumentations.
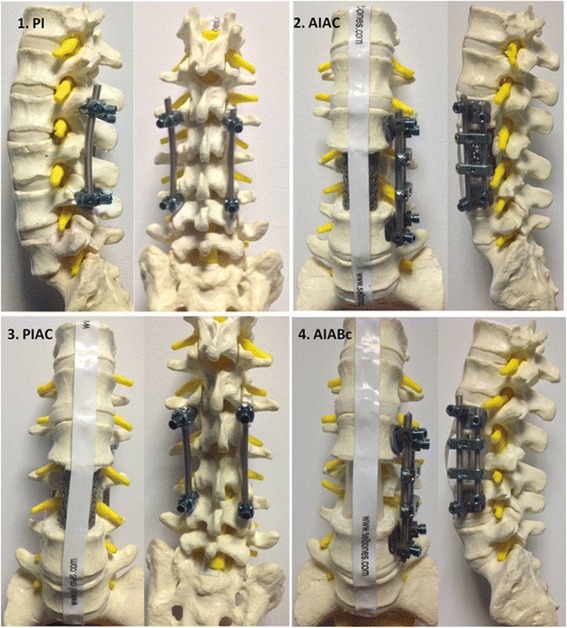
Methods: Four different spinal implant reconstruction techniques were performed using the standard sawbone lumbar vertebrae model; 1. L2-L4 posterior instrumentation without anterior column reconstruction (PI); 2. L2-L4 anterior instrumentation, L3 corpectomy, and anterior column reconstruction with a titanium cage (AIAC); 3. L2-L4 posterior instrumentation, L3 corpectomy, and anterior column reconstruction with a titanium cage (PIAC); 4. L2-L4 anterior instrumentation, L3 corpectomy, and anterior column reconstruction with chest tubes filled with bone cement (AIABc). The target was defined as the spinous process and lamina of the lumbar (L) 3 vertebra. A thermoluminescent dosimeter (TLD, LiF:Mg,Ti) was located on the measurement point anterior to the spinal cord. The prescription dose was 8 Gy and the treatment was administered in a single fraction using a CyberKnife® (Accuray Inc., Sunnyvale, CA, USA). We performed two different treatment plans. In Plan A beam interaction with the rod was not limited. In plan B the rod was considered a structure of avoidance, and interaction between the rod and beam was prevented. TLD measurements were compared with the point dose calculated by the treatment planning system (TPS).
Results and discussion: In plan A, the difference between TLD measurement and the dose calculated by the TPS was 1.7 %, 2.8 %, and 2.7 % for the sawbone with no implant, PI, and PIAC models, respectively. For the AIAC model the TLD dose was 13.8 % higher than the TPS dose; the difference was 18.6 % for the AIABc model. In plan B for the AIAC and AIABc models, TLD measurement was 2.5 % and 0.9 % higher than the dose calculated by the TPS, respectively.
Conclusions: Spinal implants may be present in the treatment field in patients scheduled to undergo SBRT. For the types of implants studied herein anterior rod instrumentation resulted in an increase in the spinal cord dose, whereas use of a titanium cage had a minimal effect on dose distribution. While planning SBRT in patients with spinal reconstructions, avoidance of the rod and preventing interaction between the rod and beam might be the optimal solution for preventing unexpectedly high spinal cord doses.
Keywords: Spinal implant; Stereotactic body radiotherapy.
Figures
References
-
- Asdourian PL, Weidenbaum M, DeWald RL, Hammerberg KW, Ramsey RG. The pattern of vertebral involvement in metastatic vertebral breast cancer. Clin Orthop Relat Res. 1990;250:164–170. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
