

Long-term survival with surgery for metachronous retroperitoneal lymph node and pancreatic metastases after curative resection of rectal cancer: a case report
- PMID: 27225417
- PMCID: PMC4880618
- DOI: 10.1186/s40792-016-0177-y
Long-term survival with surgery for metachronous retroperitoneal lymph node and pancreatic metastases after curative resection of rectal cancer: a case report
Abstract
Background: The possible benefits of the surgical resection of multiple metastases in rare sites from colorectal cancer (CRC) are still unclear. Therefore, more cases are needed to investigate the surgical outcomes of these diseases. A very rare case in which the simultaneous resection of both the metachronous retroperitoneal lymph node and pancreatic metastases from rectal cancer was successfully performed is reported.
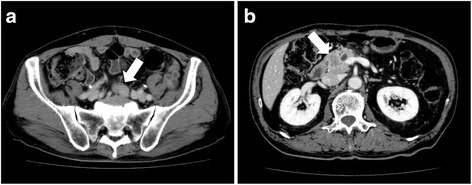
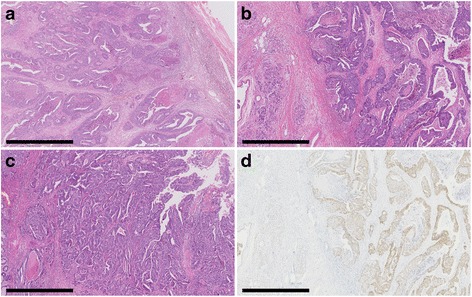
Case presentation: A 68-year-old man had undergone low anterior resection for rectal cancer. Eight months later, computed tomography showed an enlarged lymph node located below the aortic bifurcation and a pancreatic head tumor. Positron emission tomography showed increased focal uptake in these two lesions. With a diagnosis of retroperitoneal lymph node metastasis from rectal cancer and primary pancreatic cancer or pancreatic metastasis from rectal cancer, resection of the enlarged retroperitoneal lymph node and pancreaticoduodenectomy were performed. The pathological examination showed that both resected lesions were metastases from the primary rectal cancer. After the metastasectomy, the patient was given systemic chemotherapy, which was discontinued due to an adverse event. He was then followed up routinely without any medication. Sixty-nine months after the metastasectomy, he is alive without any indication of recurrence.
Conclusions: Thus, even with metastases from CRC located in rare sites, an acceptable outcome can be expected following curative surgical resection in carefully selected patients. Whenever possible, an aggressive surgical approach should be included in the multimodality treatment of metastatic CRC.
Keywords: Pancreatic metastasis; Rectal cancer; Recurrence; Retroperitoneal lymph node metastasis; Surgery.
Figures


References
-
- Abdalla EK, Vauthey JN, Ellis LM, Ellis V, Pollock R, Broglio KR, et al. Recurrence and outcomes following hepatic resection, radiofrequency ablation, and combined resection/ablation for colorectal liver metastases. Ann Surg. 2004;239:818–25. doi: 10.1097/01.sla.0000128305.90650.71. - DOI - PMC - PubMed
-
- Kato T, Yasui K, Hirai T, Kanemitsu Y, Mori T, Sugihara K, et al. Therapeutic results for hepatic metastasis of colorectal cancer with special reference to effectiveness of hepatectomy: analysis of prognostic factors for 763 cases recorded at 18 institutions. Dis Colon Rectum. 2003;46(Suppl 10):22–31. - PubMed
-
- Martin LW, Warren RS. Current management of colorectal liver metastases. Surg Oncol Clin N Am. 2000;9:853–76. - PubMed
-
- Hirosawa T, Itabashi M, Ohnuki T, Yamaguchi N, Sugihara K, Kameoka S, et al. Prognostic factors in patients undergoing complete resection of pulmonary metastases of colorectal cancer: a multi-institutional cumulative follow-up study. Surg Today. 2013;43:494–9. doi: 10.1007/s00595-012-0373-8. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
