

Elevated ventricular wall stress disrupts cardiomyocyte t-tubule structure and calcium homeostasis
- PMID: 27226008
- PMCID: PMC5031949
- DOI: 10.1093/cvr/cvw111
Elevated ventricular wall stress disrupts cardiomyocyte t-tubule structure and calcium homeostasis
Abstract
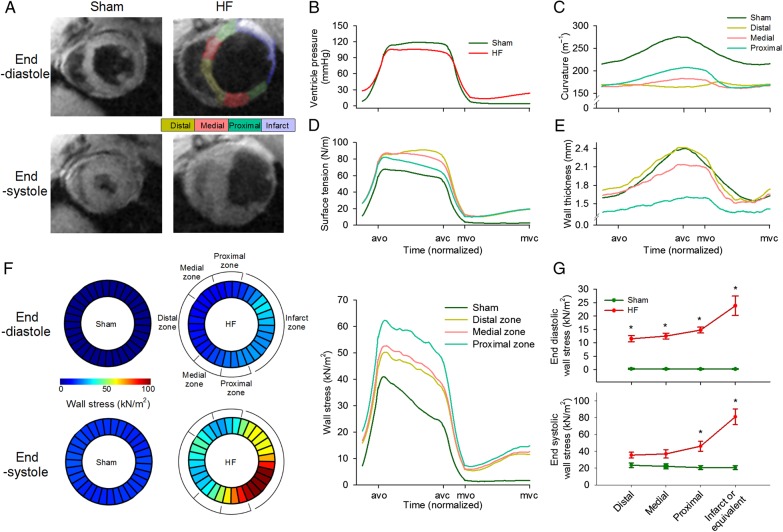
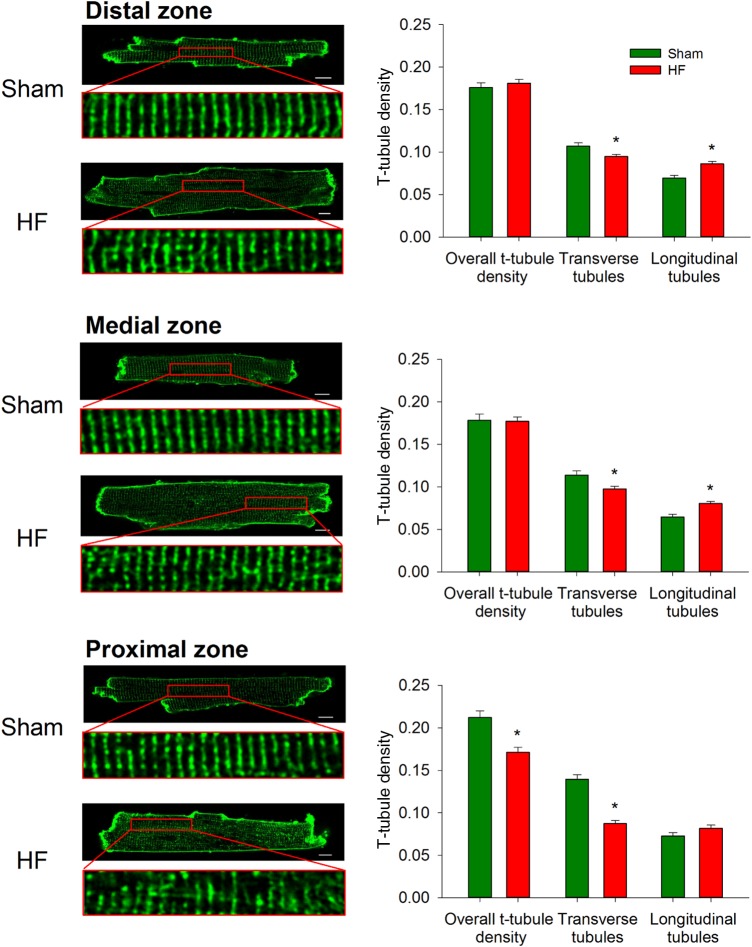
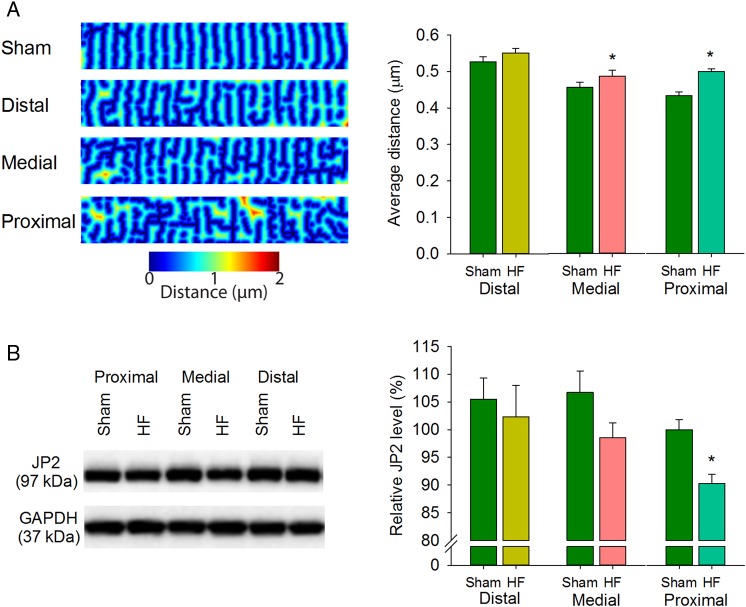
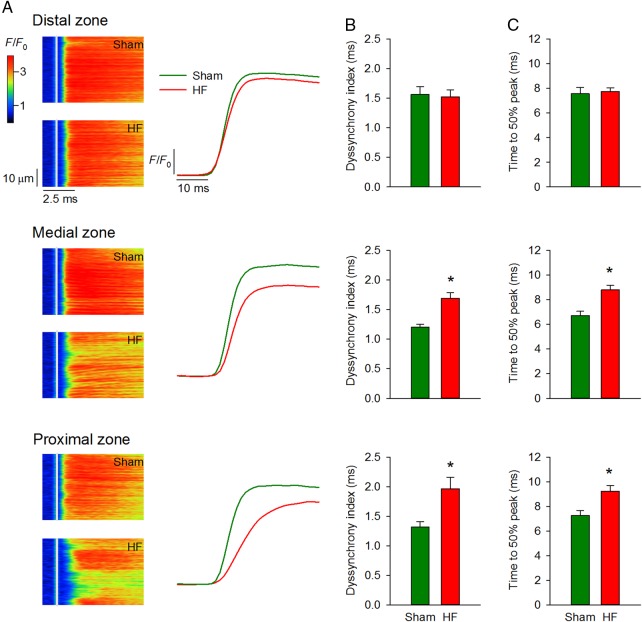
Aims: Invaginations of the cellular membrane called t-tubules are essential for maintaining efficient excitation-contraction coupling in ventricular cardiomyocytes. Disruption of t-tubule structure during heart failure has been linked to dyssynchronous, slowed Ca(2+) release and reduced power of the heartbeat. The underlying mechanism is, however, unknown. We presently investigated whether elevated ventricular wall stress triggers remodelling of t-tubule structure and function.
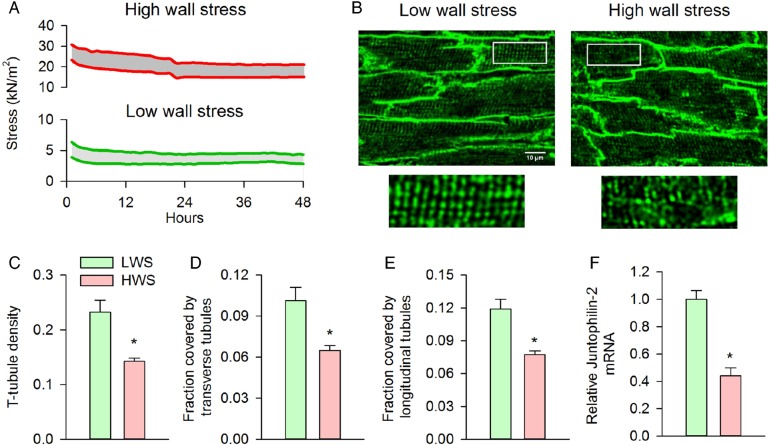
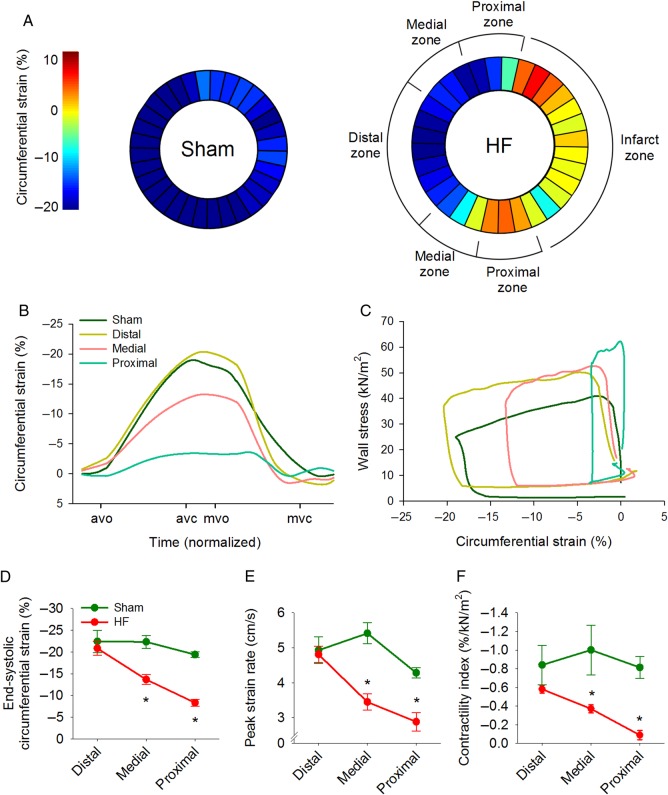
Methods and results: MRI and blood pressure measurements were employed to examine regional wall stress across the left ventricle of sham-operated and failing, post-infarction rat hearts. In failing hearts, elevated left ventricular diastolic pressure and ventricular dilation resulted in markedly increased wall stress, particularly in the thin-walled region proximal to the infarct. High wall stress in this proximal zone was associated with reduced expression of the dyadic anchor junctophilin-2 and disrupted cardiomyocyte t-tubular structure. Indeed, local wall stress measurements predicted t-tubule density across sham and failing hearts. Elevated wall stress and disrupted cardiomyocyte structure in the proximal zone were also associated with desynchronized Ca(2+) release in cardiomyocytes and markedly reduced local contractility in vivo. A causative role of wall stress in promoting t-tubule remodelling was established by applying stretch to papillary muscles ex vivo under culture conditions. Loads comparable to wall stress levels observed in vivo in the proximal zone reduced expression of junctophilin-2 and promoted t-tubule loss.
Conclusion: Elevated wall stress reduces junctophilin-2 expression and disrupts t-tubule integrity, Ca(2+) release, and contractile function. These findings provide new insight into the role of wall stress in promoting heart failure progression.
Keywords: Ca2+ homeostasis; Heart failure; Junctophilin-2; Left ventricular wall stress; T-tubules.
© The Author 2016. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Cardiac t-tubules: where structural plasticity meets functional adaptation.Cardiovasc Res. 2016 Oct;112(1):423-5. doi: 10.1093/cvr/cvw198. Cardiovasc Res. 2016. PMID: 27659500 No abstract available.
References
-
- Gomez AM, Valdivia HH, Cheng H, Lederer MR, Santana LF, Cannell MB, McCune SA, Altschuld RA, Lederer WJ. Defective excitation–contraction coupling in experimental cardiac hypertrophy and heart failure. Science 1997;276:800–806. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
