

Mechanisms of Diabetes-Induced Liver Damage: The role of oxidative stress and inflammation
- PMID: 27226903
- PMCID: PMC4868511
- DOI: 10.18295/squmj.2016.16.02.002
Mechanisms of Diabetes-Induced Liver Damage: The role of oxidative stress and inflammation
Abstract
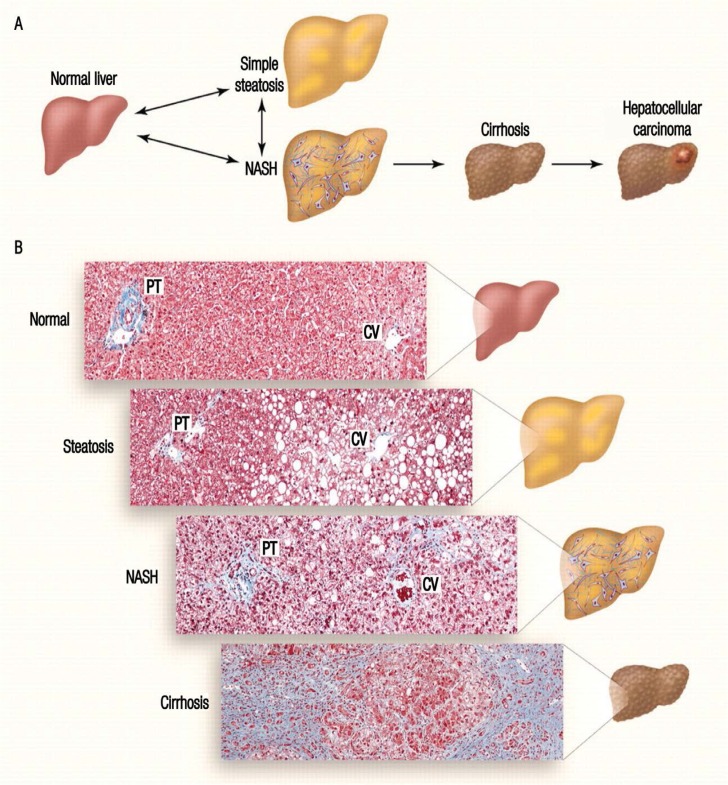
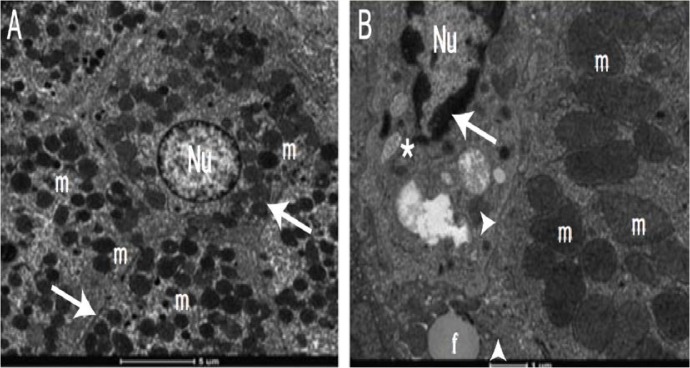
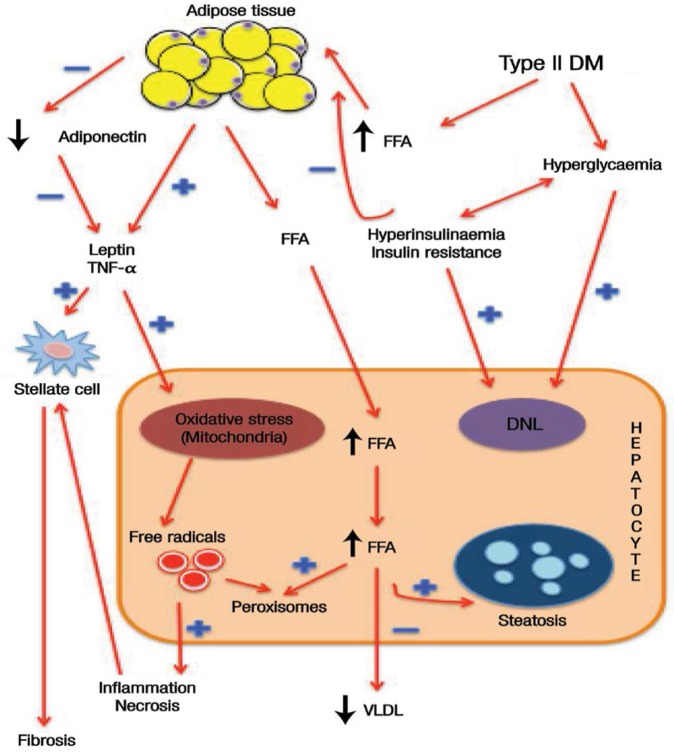
Diabetes mellitus is a non-communicable disease that occurs in both developed and developing countries. This metabolic disease affects all systems in the body, including the liver. Hyperglycaemia, mainly caused by insulin resistance, affects the metabolism of lipids, carbohydrates and proteins and can lead to non-alcoholic fatty liver disease, which can further progress to non-alcoholic steatohepatitis, cirrhosis and, finally, hepatocellular carcinomas. The underlying mechanism of diabetes that contributes to liver damage is the combination of increased oxidative stress and an aberrant inflammatory response; this activates the transcription of pro-apoptotic genes and damages hepatocytes. Significant involvement of pro-inflammatory cytokines-including interleukin (IL)-1β, IL-6 and tumour necrosis factor-α-exacerbates the accumulation of oxidative damage products in the liver, such as malondialdehyde, fluorescent pigments and conjugated dienes. This review summarises the biochemical, histological and macromolecular changes that contribute to oxidative liver damage among diabetic individuals.
Keywords: Diabetes Mellitus; Inflammation; Liver Diseases; Oxidative Stress.
Figures
References
-
- Danaei G, Finucane MM, Lu Y, Singh GM, Cowan MJ, Paciorek CJ, et al. National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: Systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2.7 million participants. Lancet. 2011;378:31–40. doi: 10.1016/s0140-6736(11)60679-x. - DOI - PubMed
-
- Reid AE. Non-alcoholic fatty liver disease. In: Feldman M, Friedman LS, Brandt LJ, editors. Sleisenger and Fordtran’s Gastrointestinal and Liver Disease: Pathophysiology/diagnosis/management. 8th ed. St Louis, Missouri, USA: Saunders; 2006. pp. 1772–99.
-
- Levinthal GN, Tavill AS. Liver disease and diabetes mellitus. Clin Diabetes. 1999;17:73.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources