

Characteristics of hyperthermia-induced hyperventilation in humans
- PMID: 27227102
- PMCID: PMC4879782
- DOI: 10.1080/23328940.2016.1143760
Characteristics of hyperthermia-induced hyperventilation in humans
Abstract
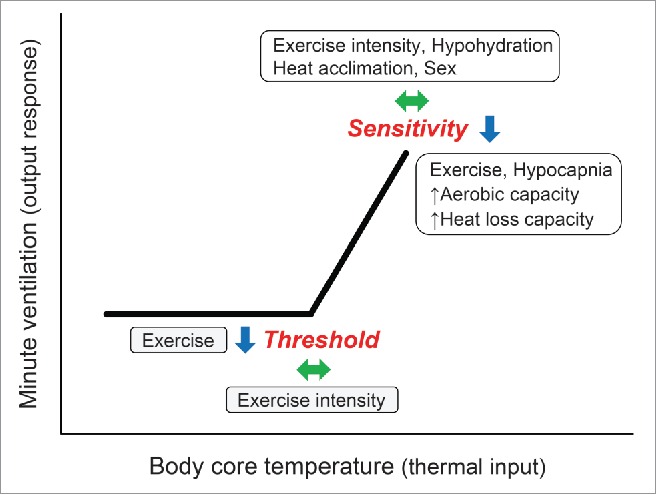
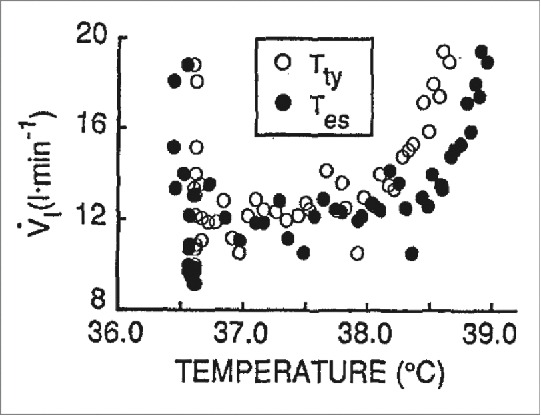
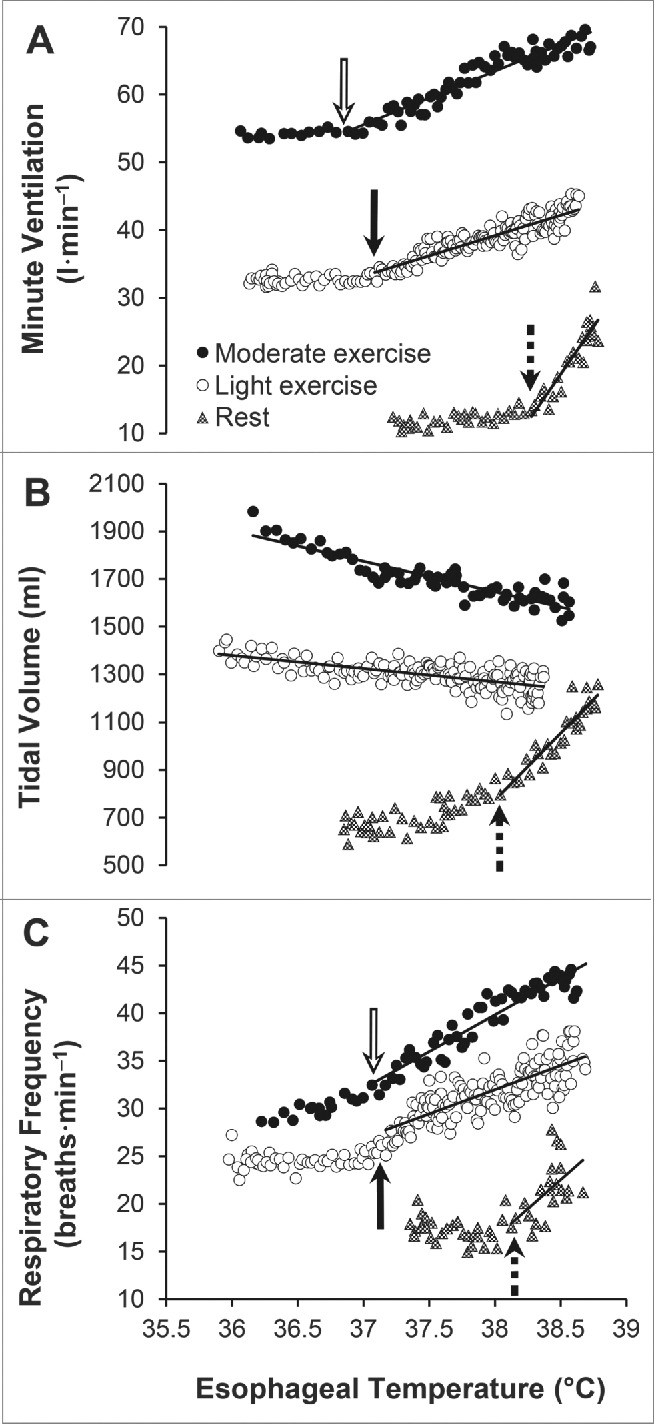
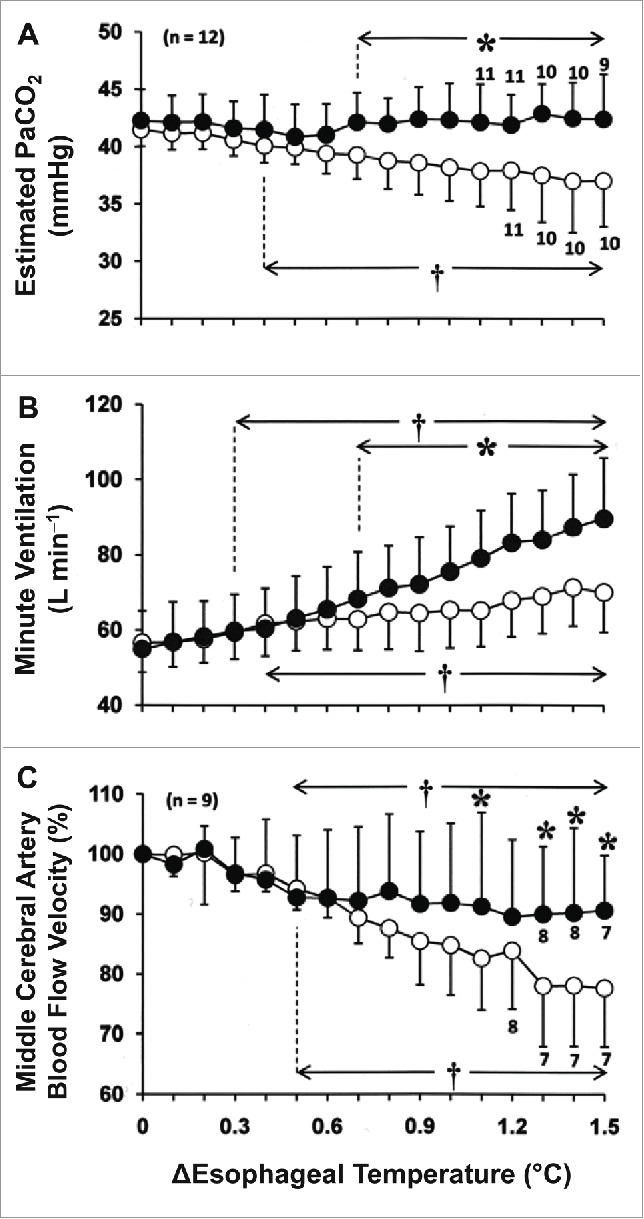
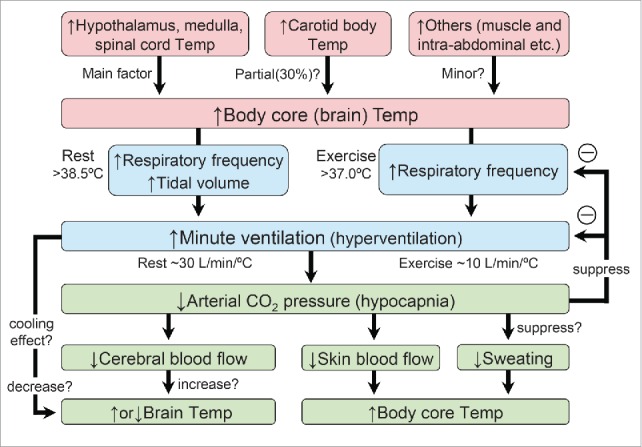
In humans, hyperthermia leads to activation of a set of thermoregulatory responses that includes cutaneous vasodilation and sweating. Hyperthermia also increases ventilation in humans, as is observed in panting dogs, but the physiological significance and characteristics of the hyperventilatory response in humans remain unclear. The relative contribution of respiratory heat loss to total heat loss in a hot environment in humans is small, and this hyperventilation causes a concomitant reduction in arterial CO2 pressure (hypocapnia), which can cause cerebral hypoperfusion. Consequently, hyperventilation in humans may not contribute to the maintenance of physiological homeostasis (i.e., thermoregulation). To gain some insight into the physiological significance of hyperthermia-induced hyperventilation in humans, in this review, we discuss 1) the mechanisms underlying hyperthermia-induced hyperventilation, 2) the factors modulating this response, and 3) the physiological consequences of the response.
Keywords: Hyperpnea; heat loss; respiratory alkalosis.
Figures
Similar articles
-
Effect of hypocapnia on the sensitivity of hyperthermic hyperventilation and the cerebrovascular response in resting heated humans.J Appl Physiol (1985). 2018 Jan 1;124(1):225-233. doi: 10.1152/japplphysiol.00232.2017. Epub 2017 Sep 28. J Appl Physiol (1985). 2018. PMID: 28970199
-
Sodium bicarbonate ingestion mitigates the heat-induced hyperventilation and reduction in cerebral blood velocity during exercise in the heat.J Appl Physiol (1985). 2021 Nov 1;131(5):1617-1628. doi: 10.1152/japplphysiol.00261.2021. Epub 2021 Sep 30. J Appl Physiol (1985). 2021. PMID: 34590911
-
Components and mechanisms of thermal hyperpnea.J Appl Physiol (1985). 2006 Aug;101(2):655-63. doi: 10.1152/japplphysiol.00210.2006. Epub 2006 Mar 24. J Appl Physiol (1985). 2006. PMID: 16565352 Review.
-
Effects of sodium bicarbonate ingestion on ventilatory and cerebrovascular responses in resting heated humans.Am J Physiol Regul Integr Comp Physiol. 2024 Oct 1;327(4):R400-R409. doi: 10.1152/ajpregu.00161.2024. Epub 2024 Aug 5. Am J Physiol Regul Integr Comp Physiol. 2024. PMID: 39102461
-
Panting as a human heat loss thermoeffector.Handb Clin Neurol. 2018;156:233-247. doi: 10.1016/B978-0-444-63912-7.00014-X. Handb Clin Neurol. 2018. PMID: 30454592 Review.
Cited by
-
Respiratory function and breathing response to water- and land-based cycling at the matched oxygen uptake.Physiol Rep. 2022 Sep;10(18):e15475. doi: 10.14814/phy2.15475. Physiol Rep. 2022. PMID: 36117322 Free PMC article.
-
Independent Predictors of Heat-Related Illness-Induced Acute Respiratory Failure: A Multicenter Cross-sectional Study.Arch Acad Emerg Med. 2025 Aug 5;13(1):e64. doi: 10.22037/aaemj.v13i1.2710. eCollection 2025. Arch Acad Emerg Med. 2025. PMID: 40801062 Free PMC article.
-
The effect of diminished metabolic acidosis on thermoregulatory response during exercise.Biol Sport. 2024 Jan;41(1):287-293. doi: 10.5114/biolsport.2024.129475. Epub 2023 Sep 20. Biol Sport. 2024. PMID: 38188109 Free PMC article.
-
The acute effect of whole-body heat therapy on peripheral and cerebral vascular reactivity in Black and White females.Microvasc Res. 2023 Jul;148:104536. doi: 10.1016/j.mvr.2023.104536. Epub 2023 Apr 5. Microvasc Res. 2023. PMID: 37024072 Free PMC article.
-
The human ventilatory response to stress: rate or depth?J Physiol. 2017 Sep 1;595(17):5729-5752. doi: 10.1113/JP274596. Epub 2017 Jul 27. J Physiol. 2017. PMID: 28650070 Free PMC article. Review.
References
-
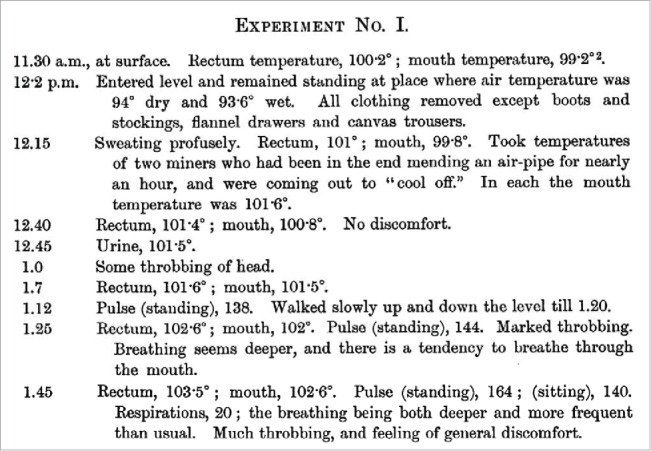
- Haldane JS. The influence of high air temperatures. J Hyg 1905; 5:494–513; PMID:20474239; http://dx.doi.org/10.1017/S0022172400006811 - DOI - PMC - PubMed
-
- Bazett HC. Studies on the effects of baths on man I. Relationship between the effects produced and the temperature of the bath. Am J Physiol 1924; 70:412–29.
-
- Bazett HC, Thurlow S, Cruwell C, Stewart W. Studies on the effects of baths on man II. The diuresis caused by warm baths, together with some observations on urinary tides. Am J Physiol 1924; 70:430–52.
-
- Cunningham DJ, O'Riordan JL. The effect of a rise in the temperature of the body on the respiratory response to carbon dioxide at rest. Q J Exp Physiol Cogn Med Sci 1957; 42:329–45; PMID:13494670 - PubMed
-
- Gaudio R Jr., Abramson N. Heat-induced hyperventilation. J Appl Physiol 1968; 25:742–6; PMID:5727201 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources