

Endoscopic ablation is a cost-effective cancer preventative therapy in patients with Barrett's esophagus who have elevated genomic instability
- PMID: 27227114
- PMCID: PMC4874803
- DOI: 10.1055/s-0042-103415
Endoscopic ablation is a cost-effective cancer preventative therapy in patients with Barrett's esophagus who have elevated genomic instability
Abstract
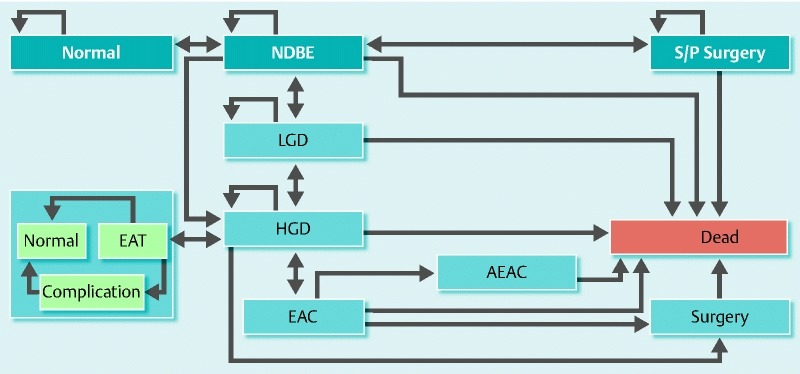
Background: The surveillance of patients with nondysplastic Barrett's esophagus (NDBE) has a high cost and is of limited effectiveness in preventing esophageal adenocarcinoma (EAC). Ablation for NDBE remains expensive and controversial. Biomarkers of genomic instability have shown promise in identifying patients with NDBE at high risk for progression to EAC. Here, we evaluate the cost-effectiveness of using such biomarkers to stratify patients with NDBE by risk for EAC and, subsequently, the cost-effectiveness of ablative therapy.
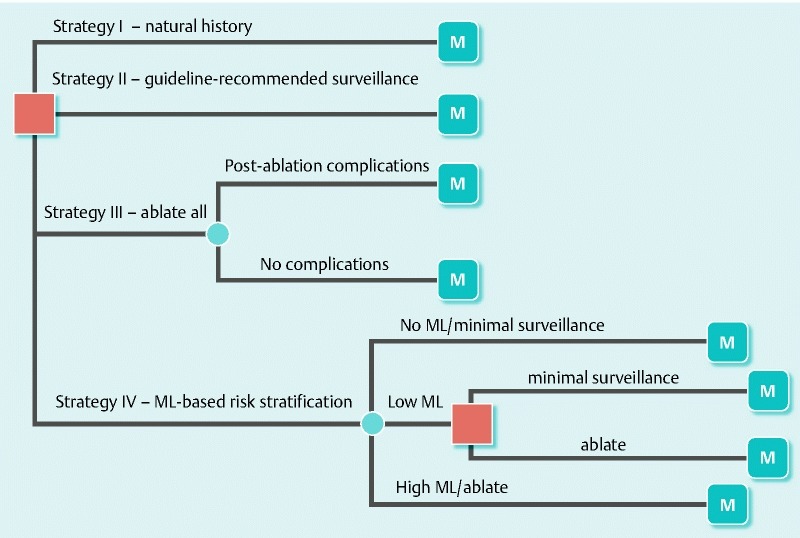
Methods: A Markov decision tree was used to evaluate four strategies in a hypothetical cohort of 50-year old patients with NDBE over their lifetime: strategy I, natural history without surveillance; strategy II, surveillance per current guidelines; strategy III, ablation for all patients; strategy IV, risk stratification with use of a biomarker panel to assess genomic instability (i. e., mutational load [ML]). Patients with no ML underwent minimal surveillance, patients with low ML underwent standard surveillance, and patients with high ML underwent ablation. The incremental cost-effectiveness ratio (ICER) and incremental net health benefit (INHB) were assessed.
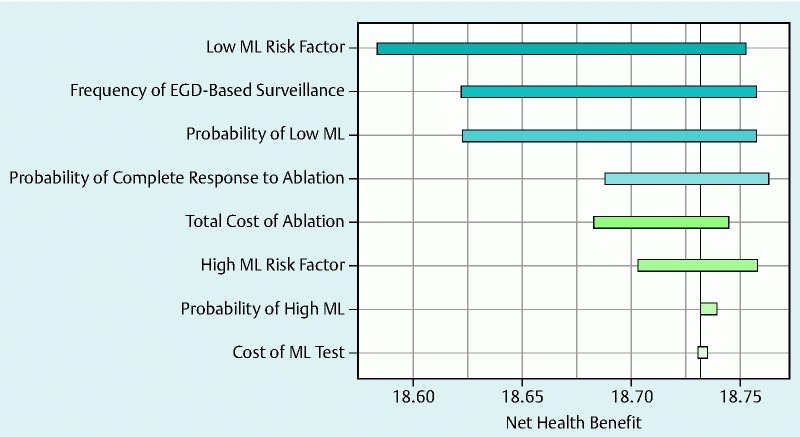
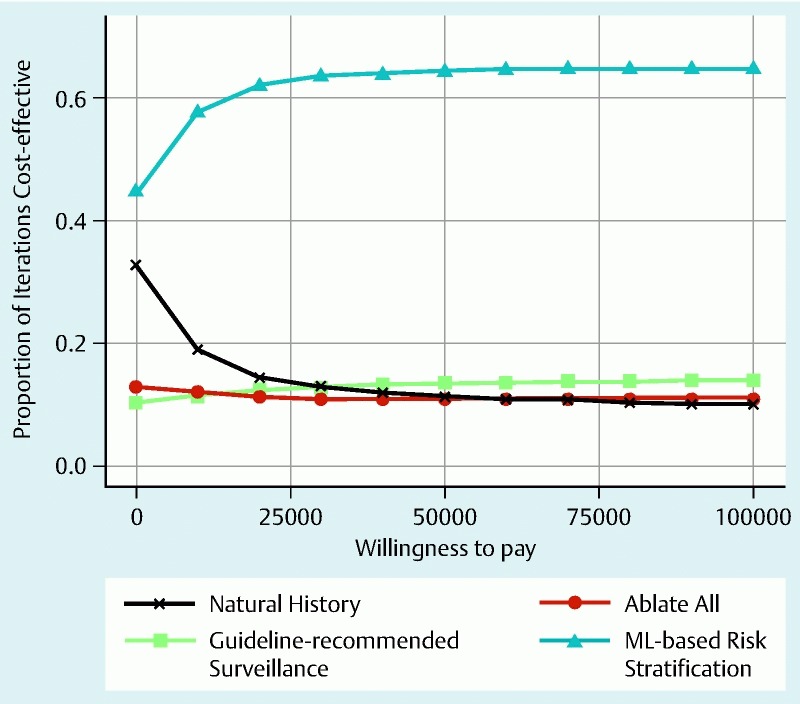
Results: Strategy IV provided the best values for quality-adjusted life years (QALYs), ICER, and INHB in comparison with strategies II and III. RESULTS were robust in sensitivity analysis. In a Monte Carlo analysis, the relative risk for the development of cancer in the patients managed with strategy IV was decreased. Critical determinants of strategy IV cost-effectiveness were the complete response rate, cost of ablation, and surveillance interval in patients with no ML.
Conclusion: The use of ML to stratify patients with NDBE by risk was the most cost-effective strategy for preventive EAC treatment. Targeting ablation toward patients with high ML presents an opportunity for a paradigm shift in the management of NDBE.
Conflict of interest statement
Figures
Similar articles
-
An economic analysis of endoscopic ablative therapy for management of nondysplastic Barrett's esophagus.Endoscopy. 2009 May;41(5):400-8. doi: 10.1055/s-0029-1214612. Epub 2009 May 5. Endoscopy. 2009. PMID: 19418393
-
The controversy regarding ablation for Barrett's esophagus without dysplasia.Curr Opin Gastroenterol. 2011 Jul;27(4):368-73. doi: 10.1097/MOG.0b013e328347bafc. Curr Opin Gastroenterol. 2011. PMID: 21577102 Review.
-
Stratification of Barrett's esophagus surveillance based on p53 immunohistochemistry: a cost-effectiveness analysis by an international collaborative group.Endoscopy. 2024 Oct;56(10):727-736. doi: 10.1055/a-2317-8184. Epub 2024 May 2. Endoscopy. 2024. PMID: 38698618
-
What is the best management strategy for high grade dysplasia in Barrett's oesophagus? A cost effectiveness analysis.Gut. 2004 Dec;53(12):1736-44. doi: 10.1136/gut.2003.033837. Gut. 2004. PMID: 15542506 Free PMC article.
-
Management of nondysplastic Barrett's esophagus: When to survey? When to ablate?Ther Adv Chronic Dis. 2022 Apr 12;13:20406223221086760. doi: 10.1177/20406223221086760. eCollection 2022. Ther Adv Chronic Dis. 2022. PMID: 35432847 Free PMC article. Review.
Cited by
-
Biomarkers of Barrett's Esophagus: From the Laboratory to Clinical Practice.Dig Dis Sci. 2018 Aug;63(8):2070-2080. doi: 10.1007/s10620-018-5088-2. Dig Dis Sci. 2018. PMID: 29713984 Free PMC article. Review.
-
Barrett's Esophagus and Esophageal Carcinoma: Can Biomarkers Guide Clinical Practice?Curr Gastroenterol Rep. 2019 Mar 12;21(4):14. doi: 10.1007/s11894-019-0685-6. Curr Gastroenterol Rep. 2019. PMID: 30868278 Review.
-
A Cost-Effectiveness Analysis Of An Adenocarcinoma Risk Prediction Multi-Biomarker Assay For Patients With Barrett's Esophagus.Clinicoecon Outcomes Res. 2019 Oct 25;11:623-635. doi: 10.2147/CEOR.S221741. eCollection 2019. Clinicoecon Outcomes Res. 2019. PMID: 31749626 Free PMC article.
References
-
- Spechler S J, Sharma P, Souza R F. et al.American Gastroenterological Association medical position statement on the management of Barrett's esophagus. Gastroenterology. 2011;140:1084–1091. - PubMed
-
- Inadomi J, Madanick R, Somsouk M. et al.Radiofrequency ablation is more cost-effective than endoscopic surveillance or esophagectomy among patients with Barrett’s esophagus and low-grade dysplasia. Gastroenterology. 2007;132:A53.
-
- Inadomi J M, Sampliner R, Lagergren J. et al.Screening and surveillance for Barrett esophagus in high-risk groups: a cost-utility analysis. Ann Intern Med. 2003;138:176–186. - PubMed
Supplemental References
-
- Maley C C, Galipeau P C, Li X. et al.The combination of genetic instability and clonal expansion predicts progression to esophageal adenocarcinoma. Cancer Res. 2004;64:7629–7633. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources