

MR Imaging Biomarkers to Monitor Early Response to Hypoxia-Activated Prodrug TH-302 in Pancreatic Cancer Xenografts
- PMID: 27227903
- PMCID: PMC4882075
- DOI: 10.1371/journal.pone.0155289
MR Imaging Biomarkers to Monitor Early Response to Hypoxia-Activated Prodrug TH-302 in Pancreatic Cancer Xenografts
Abstract
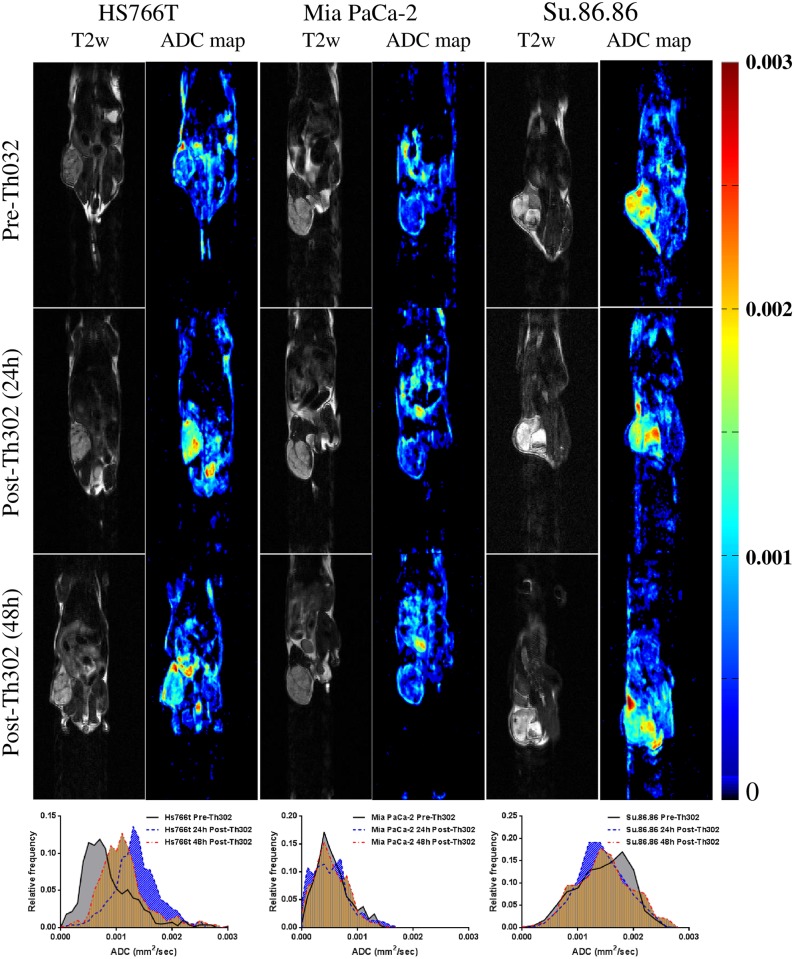
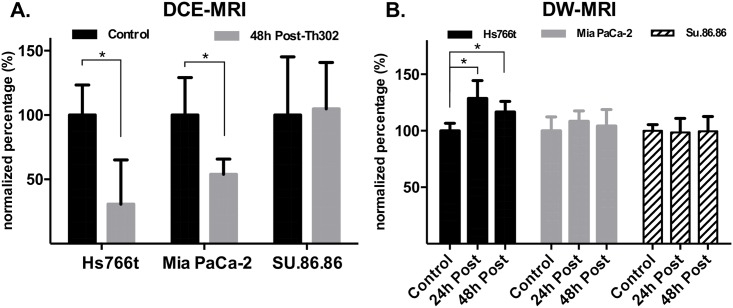
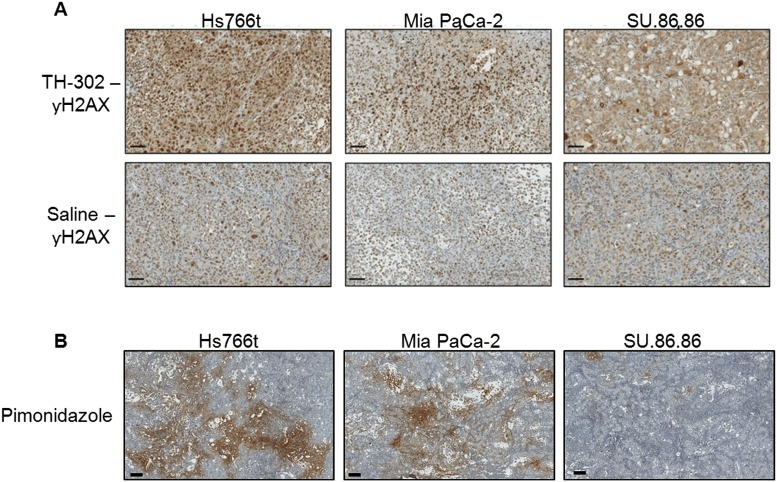
TH-302 is a hypoxia-activated prodrug known to activate selectively under the hypoxic conditions commonly found in solid tumors. It is currently being evaluated in clinical trials, including two trials in Pancreatic Ductal Adenocarcinomas (PDAC). The current study was undertaken to evaluate imaging biomarkers for prediction and response monitoring of TH-302 efficacy in xenograft models of PDAC. Dynamic contrast-enhanced (DCE) and diffusion weighted (DW) magnetic resonance imaging (MRI) were used to monitor acute effects on tumor vasculature and cellularity, respectively. Three human PDAC xenografts with known differential responses to TH-302 were imaged prior to, and at 24 h and 48 hours following a single dose of TH-302 or vehicle to determine if imaging changes presaged changes in tumor volumes. DW-MRI was performed at five b-values to generate apparent diffusion coefficient of water (ADC) maps. For DCE-MRI, a standard clinically available contrast reagent, Gd-DTPA, was used to determine blood flow into the tumor region of interest. TH-302 induced a dramatic decrease in the DCE transfer constant (Ktrans) within 48 hours after treatment in the sensitive tumors, Hs766t and Mia PaCa-2, whereas TH-302 had no effect on the perfusion behavior of resistant SU.86.86 tumors. Tumor cellularity, estimated from ADC, was significantly increased 24 and 48 hours after treatment in Hs766t, but was not observed in the Mia PaCa-2 and SU.86.86 groups. Notably, growth inhibition of Hs766t was observed immediately (day 3) following initiation of treatment, but was not observed in MiaPaCa-2 tumors until 8 days after initiation of treatment. Based on these preclinical findings, DCE-MRI measures of vascular perfusion dynamics and ADC measures of cell density are suggested as potential TH-302 response biomarkers in clinical trials.
Conflict of interest statement
Figures
Similar articles
-
Hypoxia-Activated Prodrug Evofosfamide Treatment in Pancreatic Ductal Adenocarcinoma Xenografts Alters the Tumor Redox Status to Potentiate Radiotherapy.Antioxid Redox Signal. 2021 Oct 10;35(11):904-915. doi: 10.1089/ars.2020.8131. Epub 2020 Sep 15. Antioxid Redox Signal. 2021. PMID: 32787454 Free PMC article.
-
Metabolic and Physiologic Imaging Biomarkers of the Tumor Microenvironment Predict Treatment Outcome with Radiation or a Hypoxia-Activated Prodrug in Mice.Cancer Res. 2018 Jul 15;78(14):3783-3792. doi: 10.1158/0008-5472.CAN-18-0491. Epub 2018 May 23. Cancer Res. 2018. PMID: 29792309 Free PMC article.
-
Imaging biomarkers to monitor response to the hypoxia-activated prodrug TH-302 in the MiaPaCa2 flank xenograft model.Magn Reson Imaging. 2012 Sep;30(7):1002-9. doi: 10.1016/j.mri.2012.02.015. Epub 2012 May 1. Magn Reson Imaging. 2012. PMID: 22554971 Free PMC article.
-
Evofosfamide, a new horizon in the treatment of pancreatic cancer.Anticancer Drugs. 2016 Sep;27(8):723-5. doi: 10.1097/CAD.0000000000000386. Anticancer Drugs. 2016. PMID: 27232101 Review.
-
DCE-MRI of Tumor Hypoxia and Hypoxia-Associated Aggressiveness.Cancers (Basel). 2020 Jul 20;12(7):1979. doi: 10.3390/cancers12071979. Cancers (Basel). 2020. PMID: 32698525 Free PMC article. Review.
Cited by
-
Hypoxia-Activated Prodrug Evofosfamide Treatment in Pancreatic Ductal Adenocarcinoma Xenografts Alters the Tumor Redox Status to Potentiate Radiotherapy.Antioxid Redox Signal. 2021 Oct 10;35(11):904-915. doi: 10.1089/ars.2020.8131. Epub 2020 Sep 15. Antioxid Redox Signal. 2021. PMID: 32787454 Free PMC article.
-
Imaging of glucose metabolism by 13C-MRI distinguishes pancreatic cancer subtypes in mice.Elife. 2019 Aug 13;8:e46312. doi: 10.7554/eLife.46312. Elife. 2019. PMID: 31408004 Free PMC article.
-
Radiotherapy Synergizes with the Hypoxia-Activated Prodrug Evofosfamide: In Vitro and In Vivo Studies.Antioxid Redox Signal. 2018 Jan 10;28(2):131-140. doi: 10.1089/ars.2017.7106. Epub 2017 Sep 8. Antioxid Redox Signal. 2018. PMID: 28741367 Free PMC article.
-
Multiparametric MRI and Coregistered Histology Identify Tumor Habitats in Breast Cancer Mouse Models.Cancer Res. 2019 Aug 1;79(15):3952-3964. doi: 10.1158/0008-5472.CAN-19-0213. Epub 2019 Jun 11. Cancer Res. 2019. PMID: 31186232 Free PMC article.
-
Toward diffusion MRI in the diagnosis and treatment of pancreatic cancer.Med Oncol. 2025 May 28;42(7):222. doi: 10.1007/s12032-025-02759-5. Med Oncol. 2025. PMID: 40434720 Review.
References
-
- Angst E, Kim-Fuchs C, Kuruvilla YC, Inderbitzin D, Montani M, Candinas D, et al. How to counter the problem of R1 resection in duodenopancreatectomy for pancreatic cancer? Journal of gastrointestinal surgery: official journal of the Society for Surgery of the Alimentary Tract. 2012;16(3):673 Epub 2012/01/11. 10.1007/s11605-011-1791-4 . - DOI - PubMed
-
- Campbell F, Smith RA, Whelan P, Sutton R, Raraty M, Neoptolemos JP, et al. Classification of R1 resections for pancreatic cancer: the prognostic relevance of tumour involvement within 1 mm of a resection margin. Histopathology. 2009;55(3):277–83. Epub 2009/09/03. 10.1111/j.1365-2559.2009.03376.x . - DOI - PubMed
-
- Ferrone CR, Brennan MF, Gonen M, Coit DG, Fong Y, Chung S, et al. Pancreatic adenocarcinoma: the actual 5-year survivors. Journal of gastrointestinal surgery: official journal of the Society for Surgery of the Alimentary Tract. 2008;12(4):701–6. Epub 2007/11/21. 10.1007/s11605-007-0384-8 . - DOI - PubMed
-
- Howard TJ, Krug JE, Yu J, Zyromski NJ, Schmidt CM, Jacobson LE, et al. A margin-negative R0 resection accomplished with minimal postoperative complications is the surgeon's contribution to long-term survival in pancreatic cancer. Journal of gastrointestinal surgery: official journal of the Society for Surgery of the Alimentary Tract. 2006;10(10):1338–45; discussion 45–6. Epub 2006/12/19. 10.1016/j.gassur.2006.09.008 . - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
