

Should Splenic Hilar Lymph Nodes be Dissected for Siewert Type II and III Esophagogastric Junction Carcinoma Based on Tumor Diameter?: A Retrospective Database Analysis
- PMID: 27227913
- PMCID: PMC4902337
- DOI: 10.1097/MD.0000000000003473
Should Splenic Hilar Lymph Nodes be Dissected for Siewert Type II and III Esophagogastric Junction Carcinoma Based on Tumor Diameter?: A Retrospective Database Analysis
Abstract
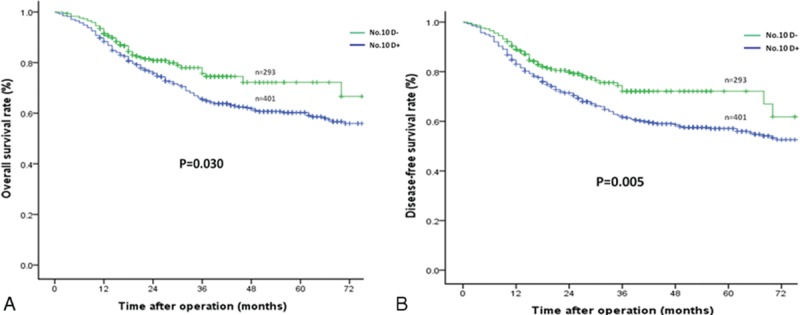
The aim of the study is to identify the value of a spleen-preserving No. 10 lymphadenectomy (SPL) for Siewert type II/III adenocarcinoma of the esophagogastric junction (AEG).From January 2007 to June 2014, 694 patients undergoing radical total gastrectomy for Siewert type II/III AEG were analyzed. Oncologic outcomes were compared between SPL and no SPL (No. 10D+ and No. 10D-) groups.The incidence of No. 10 lymph node metastasis (LNM) was 12.3%. No significant differences in the incidence of No. 10 LNM were found between Siewert type II AEG with tumor diameters of <4 cm and ≥4 cm (P = 0.071). However, Siewert type III AEG with a tumor diameter ≥4 cm showed a significantly higher frequency of No. 10 LNM compared with a tumor diameter <4 cm (P < 0.001). The No. 10D+ group had superior 3-year overall survival (OS) and disease-free survival (DFS) rates compared with the No. 10D- group (P = 0.030 and P = 0.005, respectively). For patients with Siewert type II and type III AEG with a tumor diameter <4 cm, the 3-year OS and DFS rates were similar between the 2 groups. However, the No. 10D+ group had better 3-year OS (66.6% vs 51.1%, P = 0.019) and DFS (63.2% vs 45.9%, P = 0.007) rates for Siewert type III AEG with a tumor diameter ≥4 cm. A multivariate Cox regression showed that SPL was an independent prognostic factor in Siewert type III AEG with a tumor diameter ≥4 cm.SPL may improve the prognosis of Siewert type III AEG with a tumor diameter ≥4 cm, whereas SPL may be omitted without decreasing survival in patients with Siewert type II or type III AEG with a tumor diameter <4 cm.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures



Similar articles
-
Clinical significance of lower perigastric lymph nodes dissection in Siewert type II/III adenocarcinoma of esophagogastric junction: a retrospective propensity score matched study.Langenbecks Arch Surg. 2022 May;407(3):985-998. doi: 10.1007/s00423-021-02380-w. Epub 2021 Nov 18. Langenbecks Arch Surg. 2022. PMID: 34792614
-
Should Pyloric Lymph Nodes Be Dissected for Siewert Type II and III Adenocarcinoma of the Esophagogastric Junctions: Experience from a High-Volume Center in China.J Gastrointest Surg. 2019 Feb;23(2):256-263. doi: 10.1007/s11605-018-3935-2. Epub 2018 Oct 17. J Gastrointest Surg. 2019. PMID: 30334176
-
Assessment of risk factors of lymph node metastasis and prognosis of Siewert II/III adenocarcinoma of esophagogastric junction: A retrospective study.Medicine (Baltimore). 2024 Mar 1;103(9):e37289. doi: 10.1097/MD.0000000000037289. Medicine (Baltimore). 2024. PMID: 38428860 Free PMC article.
-
Laparoscopic versus Open Approach for Siewert Type II/III Adenocarcinoma of the Esophagogastric Junction: A Systematic Review and Meta-Analysis.Dig Surg. 2022;39(5-6):210-223. doi: 10.1159/000528912. Epub 2023 Jan 4. Dig Surg. 2022. PMID: 36599323
-
Incidence of lymph node metastasis at each station in Siewert types Ⅱ/Ⅲ adenocarcinoma of the esophagogastric junction: A systematic review and meta-analysis.Surg Oncol. 2020 Dec;35:62-70. doi: 10.1016/j.suronc.2020.08.001. Epub 2020 Aug 13. Surg Oncol. 2020. PMID: 32835903
Cited by
-
Survival Benefit of Pyloric Lymph Node Dissection for Siewert Type II/III Adenocarcinoma of the Esophagogastric Junction Based on Tumor Diameter: A Large Cohort Study.Front Oncol. 2021 Dec 1;11:748694. doi: 10.3389/fonc.2021.748694. eCollection 2021. Front Oncol. 2021. PMID: 34926257 Free PMC article.
-
Trends in esophageal and esophagogastric junction cancer research from 2007 to 2016: A bibliometric analysis.Medicine (Baltimore). 2017 May;96(20):e6924. doi: 10.1097/MD.0000000000006924. Medicine (Baltimore). 2017. PMID: 28514311 Free PMC article. Review.
-
Priority of lymph node dissection for advanced esophagogastric junction adenocarcinoma with the tumor center located below the esophagogastric junction.Medicine (Baltimore). 2019 Dec;98(51):e18451. doi: 10.1097/MD.0000000000018451. Medicine (Baltimore). 2019. PMID: 31861019 Free PMC article.
-
Feasibility of laparoscopic gastrectomy for patients with Siewert-type II/III adenocarcinoma of the esophagogastric junction: A propensity score matching analysis.PLoS One. 2018 Sep 26;13(9):e0203125. doi: 10.1371/journal.pone.0203125. eCollection 2018. PLoS One. 2018. PMID: 30256806 Free PMC article.
-
Laparoscopic splenic hilar lymph node dissection for advanced gastric cancer: to be or not to be.Ann Transl Med. 2019 Jul;7(14):343. doi: 10.21037/atm.2019.07.35. Ann Transl Med. 2019. PMID: 31475213 Free PMC article. Review.
References
-
- Vial M, Grande L, Pera M. Epidemiology of adenocarcinoma of the esophagus, gastric cardia, and upper gastric third. Recent Results Cancer Res 2010; 182:1–17. - PubMed
-
- Siewert JR, Stein HJ. Classification of adenocarcinoma of the oesophagogastric junction. Br J Surg 1998; 85:1457–1459. - PubMed
-
- Meier I, Merkel S, Papadopoulos T, et al. Adenocarcinoma of the esophagogastric junction: the pattern of metastatic lymph node dissemination as a rationale for elective lymphatic target volume definition. Int J Radiat Oncol Biol Phys 2008; 70:1408–1417. - PubMed
-
- Fang WL, Wu CW, Chen JH, et al. Esophagogastric junction adenocarcinoma according to Siewert classification in Taiwan. Ann Surg Oncol 2009; 16:3237–3244. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
