

Differences Between the "Chinese AMS Score" and the Lake Louise Score in the Diagnosis of Acute Mountain Sickness
- PMID: 27227918
- PMCID: PMC4902342
- DOI: 10.1097/MD.0000000000003512
Differences Between the "Chinese AMS Score" and the Lake Louise Score in the Diagnosis of Acute Mountain Sickness
Abstract
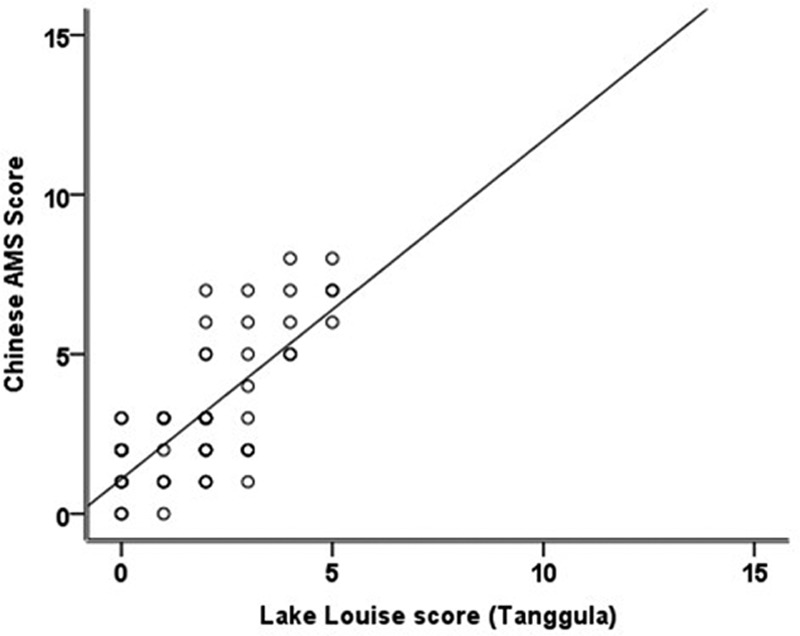
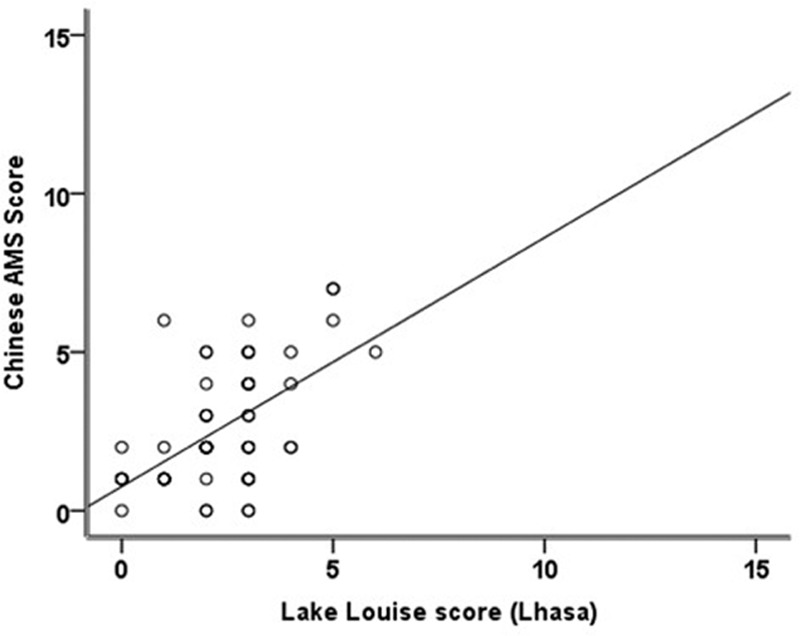
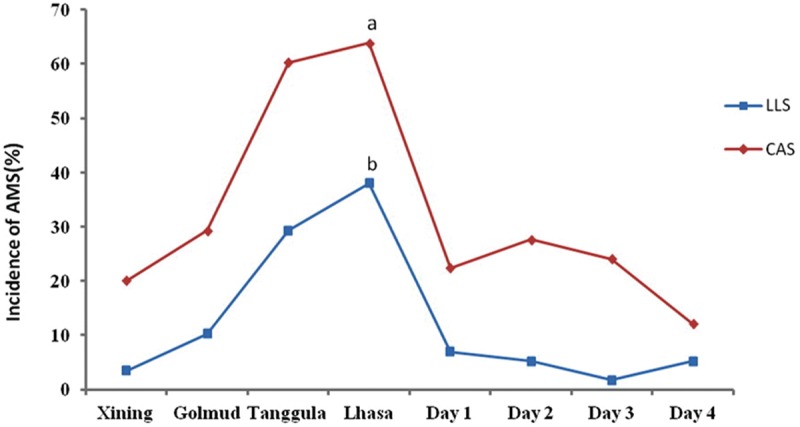
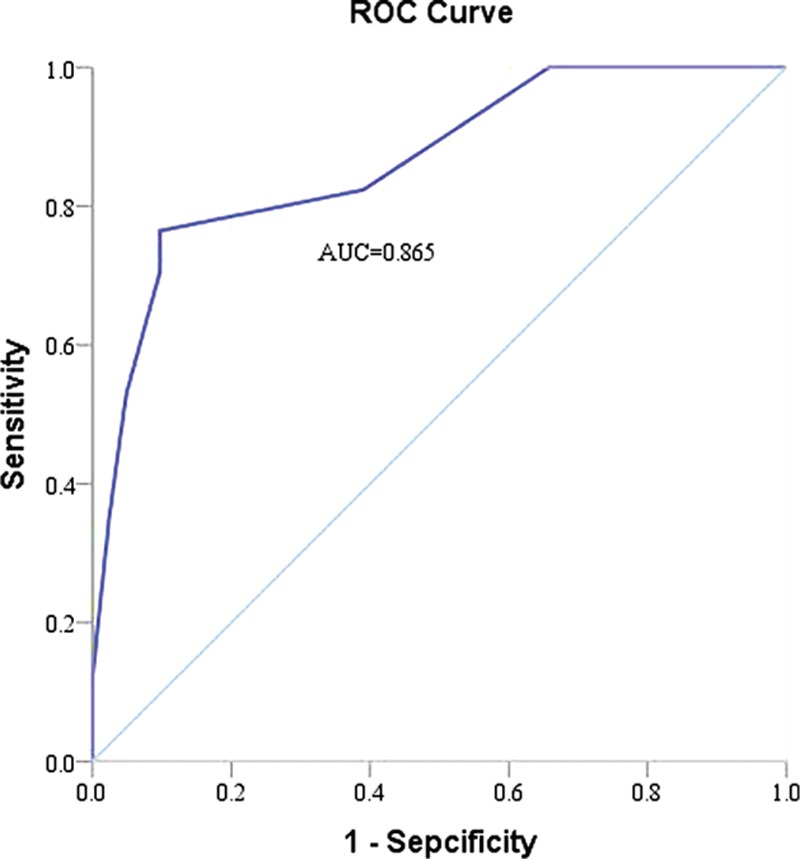
The Chinese AMS score (CAS) is used in clinical medicine and research to diagnosis acute mountain sickness (AMS). However, the Lake Louise Score (LLS) is the well-accepted standard for diagnosing AMS. The difference between the CAS and LLS questionnaires is that the CAS considers more nonspecific symptoms. The aim of the present study was to evaluate differences in AMS prevalence according to the LLS and CAS criteria. We surveyed 58 males who traveled from Chongqing (300 m) to Lhasa (3658 m) via the Qinghai-Tibet train. Cases of AMS were diagnosed using LLS and CAS questionnaires in a few railway stations at different evaluation areas along the road. We subsequently evaluated discrepancies in values related to the prevalence of AMS determined using the 2 types of questionnaires (CAS and LLS). The prevalence of CAS-diagnosed AMS indicated that the percentage of AMS cases among the 58 young men was 29.3% in Golmud, 60.3% in Tanggula, 63.8% in Lhasa, 22.4% on the first day after arrival in Lhasa, 27.6% on the second day, 24.1% on the third day, and 12.1% on the fourth day. The prevalence of LLS-diagnosed AMS in Golmud was 10.3%, 38% in Lhasa, and 6.9% on day 1, the prevalence in each station was lower than that as assessed by the CAS. Our experimental data indicate that AMS diagnoses ascertained using the CAS indicate a higher AMS prevalence than those ascertained using the LLS. Through statistical analysis, the CAS seems capable of effectively diagnosing AMS as validated by LLS (sensitivity 61.8%, specificity 92.7%).
Conflict of interest statement
The authors state that there are no conflicts of interest regarding the publication of this article and that there are no financial ties to disclose.
Figures
Similar articles
-
Assessment of Acute Mountain Sickness: Comparing the Chinese AMS Score to the Lake Louise Score.High Alt Med Biol. 2024 Sep;25(3):164-173. doi: 10.1089/ham.2023.0033. Epub 2024 Apr 11. High Alt Med Biol. 2024. PMID: 38602430
-
[Changes in oxygen saturation can not help diagnose acute mountain sickness (AMS): ascending to Lhasa on the Qinghai-Tibet train].Zhongguo Ying Yong Sheng Li Xue Za Zhi. 2016 Jun 8;32(6):519-524. doi: 10.13459/j.cnki.cjap.2016.06.008. Zhongguo Ying Yong Sheng Li Xue Za Zhi. 2016. PMID: 29926619 Chinese.
-
Incidence of acute mountain sickness in young adults at 3200 meters: comparison of the Lake Louise Scoring and Chinese Scoring Systems.Genet Mol Res. 2013 Dec 16;12(4):6790-801. doi: 10.4238/2013.December.16.5. Genet Mol Res. 2013. PMID: 24391027
-
The 2018 Lake Louise Acute Mountain Sickness Score.High Alt Med Biol. 2018 Mar;19(1):4-6. doi: 10.1089/ham.2017.0164. Epub 2018 Mar 13. High Alt Med Biol. 2018. PMID: 29583031 Free PMC article.
-
Association between acute mountain sickness (AMS) and age: a meta-analysis.Mil Med Res. 2018 May 11;5(1):14. doi: 10.1186/s40779-018-0161-x. Mil Med Res. 2018. PMID: 29747689 Free PMC article. Review.
Cited by
-
Metabolite and protein shifts in mature erythrocyte under hypoxia.iScience. 2024 Feb 23;27(4):109315. doi: 10.1016/j.isci.2024.109315. eCollection 2024 Apr 19. iScience. 2024. PMID: 38487547 Free PMC article. Review.
-
A study of survival strategies for improving acclimatization of lowlanders at high-altitude.Heliyon. 2023 Mar 28;9(4):e14929. doi: 10.1016/j.heliyon.2023.e14929. eCollection 2023 Apr. Heliyon. 2023. PMID: 37025911 Free PMC article. Review.
-
Exploring the Blood Biomarkers and Potential Therapeutic Agents for Human Acute Mountain Sickness Based on Transcriptomic Analysis, Inflammatory Infiltrates and Molecular Docking.Int J Mol Sci. 2024 Oct 21;25(20):11311. doi: 10.3390/ijms252011311. Int J Mol Sci. 2024. PMID: 39457093 Free PMC article.
References
-
- Hackett PH, Roach RC. High-altitude illness. N Engl J Med 2001; 345:107–114. - PubMed
-
- Luo Y, Yang X, Gao Y. Strategies for the prevention of acute mountain sickness and treatment for large groups making a rapid ascent in China. Int J Cardiol 2013; 169:97–100. - PubMed
-
- Murdoch DR. Altitude illness among tourists flying to 3740 meters elevation in the Nepal Himalayas. J Travel Med 1995; 2:255–256. - PubMed
-
- Roach RC, Bartsch P, Hackett PH, et al. The Lake Louise acute mountain-sickness scoring system//Sutton JR, Houston CS, Coates. Hypoxia and Mountain Medicine. Vt, Burlington: Queen City Press, 1993:272–274.
-
- Maggiorini M, Muller A, Hofstetter D, et al. Assessment of acute mountain sickness by different score protocols in the Swiss Alps. Aviat Space Environ Med 1998; 69:1186–1192. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
