

Assessment of The Lymphatic System of the Genitalia Using Magnetic Resonance Lymphography Before and After Treatment of Male Genital Lymphedema
- PMID: 27227943
- PMCID: PMC4902367
- DOI: 10.1097/MD.0000000000003755
Assessment of The Lymphatic System of the Genitalia Using Magnetic Resonance Lymphography Before and After Treatment of Male Genital Lymphedema
Abstract
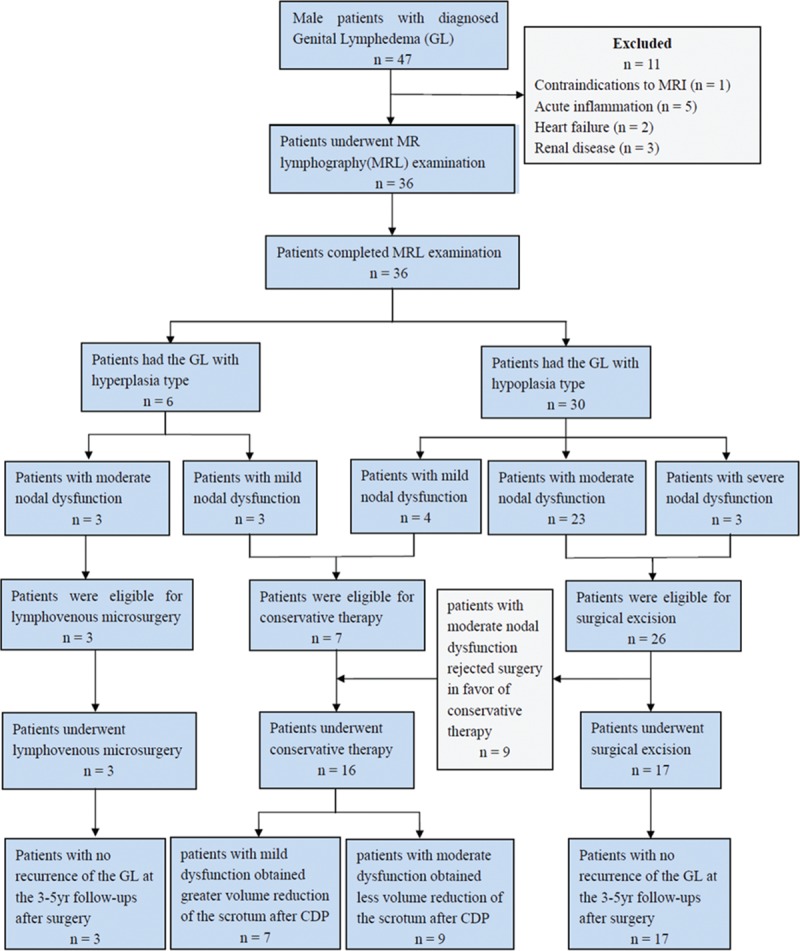
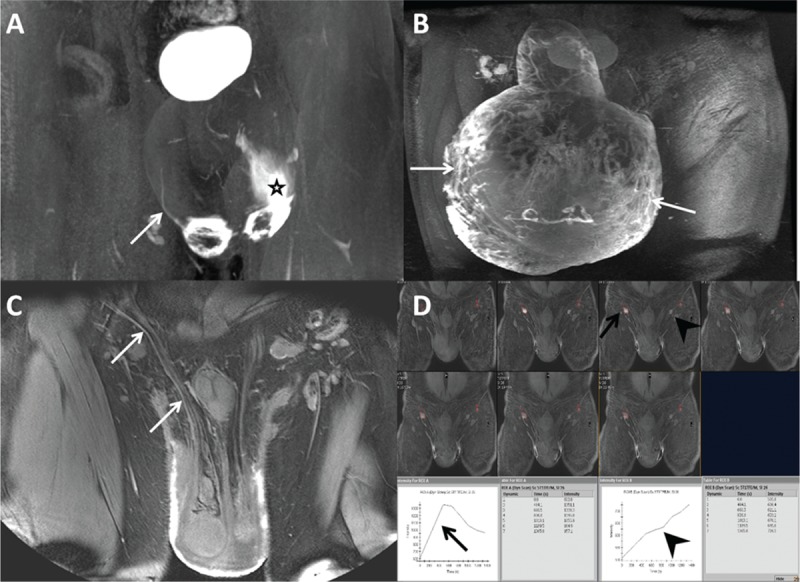
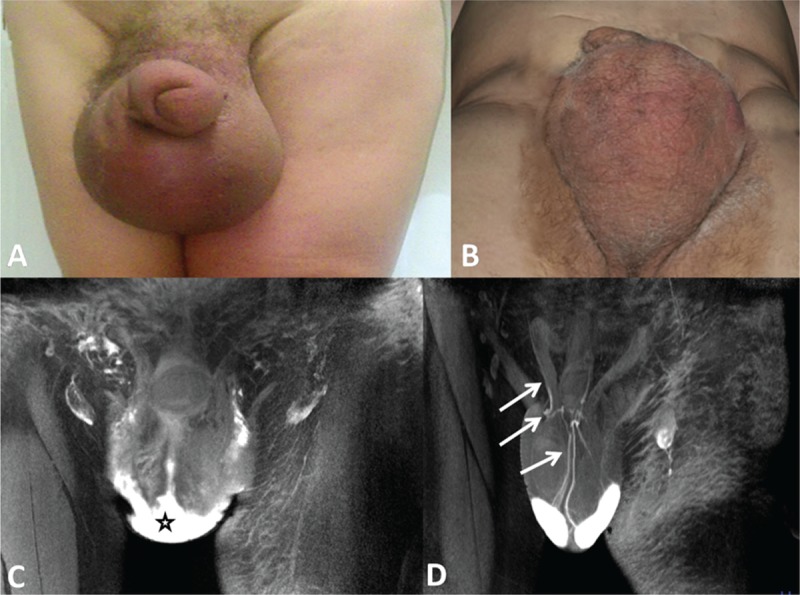
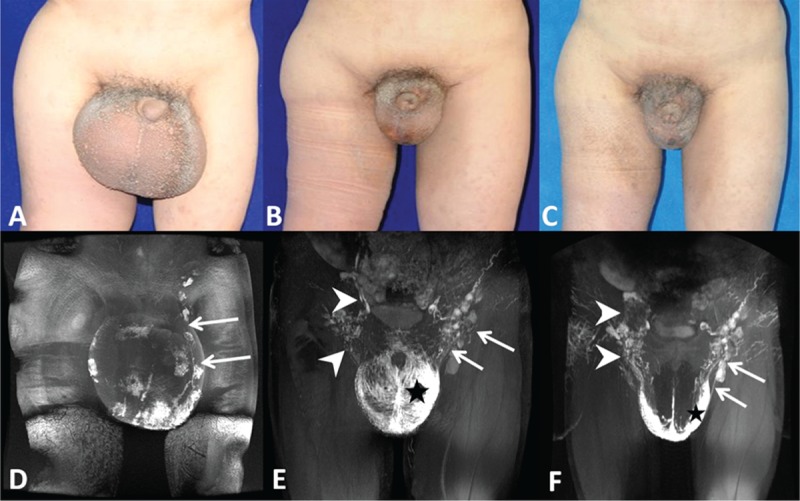
Treatment for chronic male genital lymphedema (GL) is limited. No standard treatment or validated instrument to assess GL is available. The aim of this study was to explore whether magnetic resonance lymphography (MRL) could be used to assess GL, select proper treatment for patients, and monitor postoperative progress.This is a retrospective analysis of a prospectively acquired cohort of men with GL presenting for MRL over a 7-year period. Thirty-six of 47 eligible men were included. All men were offered preoperative and postoperative MRL and assigned a morphology and function classification. Men with mild, moderate, and severe nodal dysfunction underwent complex decongestive physiotherapy (CDP), lymphoveneous microsurgery, and surgical excision, respectively. The volume reductions in the genitalia of patients with mild and moderate nodal dysfunction were recorded and compared using Student t test.The abnormal superficial and deep lymphatic vessels in the lymphedematous genitalia were detected by MRL, and inguinal lymph node dysfunction was classified by MRL. Seven patients with mild dysfunction who underwent CDP showed a more significant mean volume reduction in the genitalia than did 9 patients with moderate dysfunction. Three patients with hyperplasia and moderate dysfunction who underwent microsurgical operations and 17 patients with hypoplasia and moderate or severe nodal dysfunction who underwent surgical excision had excellent cosmetic results with no lymphedema at the 3- to 5-year follow-up.MRL can be used to assess morphological and functional lymphatic abnormalities in GL, preoperatively select appropriate treatment, and postoperatively evaluate treatment outcomes.
Figures
Similar articles
-
Magnetic Resonance Lymphography at 9.4 T Using a Gadolinium-Based Nanoparticle in Rats: Investigations in Healthy Animals and in a Hindlimb Lymphedema Model.Invest Radiol. 2017 Dec;52(12):725-733. doi: 10.1097/RLI.0000000000000398. Invest Radiol. 2017. PMID: 28678084
-
Magnetic resonance lymphography as three-dimensional navigation for lymphaticovenular anastomosis in patients with leg lymphedema.J Plast Reconstr Aesthet Surg. 2021 Jun;74(6):1253-1260. doi: 10.1016/j.bjps.2020.10.099. Epub 2020 Nov 8. J Plast Reconstr Aesthet Surg. 2021. PMID: 33277216
-
Could MRI visualize the invisible? An Italian single center study comparing magnetic resonance lymphography (MRL), super microsurgery and histology in the identification of lymphatic vessels.Eur Rev Med Pharmacol Sci. 2017 Feb;21(4):687-694. Eur Rev Med Pharmacol Sci. 2017. PMID: 28272715
-
A systematic review of magnetic resonance lymphography for the evaluation of peripheral lymphedema.J Vasc Surg Venous Lymphat Disord. 2020 Sep;8(5):882-892.e2. doi: 10.1016/j.jvsv.2020.03.007. Epub 2020 May 13. J Vasc Surg Venous Lymphat Disord. 2020. PMID: 32417145
-
A Meta-analysis of 37 Studies on the Effectiveness of Microsurgical Techniques for Lymphedema.Ann Vasc Surg. 2022 Oct;86:440-451.e6. doi: 10.1016/j.avsg.2022.04.038. Epub 2022 May 16. Ann Vasc Surg. 2022. PMID: 35589027 Review.
Cited by
-
Surgical reconstruction of massive scrotal lymphedema associated with hidradenitis suppurativa: a case report.Gland Surg. 2021 May;10(5):1800-1805. doi: 10.21037/gs-20-460. Gland Surg. 2021. PMID: 34164324 Free PMC article.
-
Surgical reconstruction of primary genital lymphedema-long term therapeutic efficacy.Gland Surg. 2020 Apr;9(2):575-581. doi: 10.21037/gs.2020.03.19. Gland Surg. 2020. PMID: 32420292 Free PMC article.
-
MRI of Lymphedema.J Magn Reson Imaging. 2023 Apr;57(4):977-991. doi: 10.1002/jmri.28496. Epub 2022 Oct 22. J Magn Reson Imaging. 2023. PMID: 36271779 Free PMC article. Review.
-
Effects of Ultrasound-guided Lower Abdominal Lymphaticovenous Anastomosis on Lower Abdominal Lymphedema.Plast Reconstr Surg Glob Open. 2023 Dec 13;11(12):e5443. doi: 10.1097/GOX.0000000000005443. eCollection 2023 Dec. Plast Reconstr Surg Glob Open. 2023. PMID: 38093725 Free PMC article.
-
Genital Lymphedema after Cancer Treatment: A Narrative Review.Cancers (Basel). 2022 Nov 25;14(23):5809. doi: 10.3390/cancers14235809. Cancers (Basel). 2022. PMID: 36497291 Free PMC article. Review.
References
-
- Moffatt CJ, Franks PJ, Doherty DC, et al. Lymphoedema: an underestimated health problem. QJM 2003; 96:731–738. - PubMed
-
- Dandapat MC, Mohapatro SK, Patro SK. Elephantiasis of the penis and scrotum. A review of 350 cases. Am J Surg 1985; 149:686–690. - PubMed
-
- Sauer PF, Bueschen AJ, Vasconez LO. Lymphedema of the penis and scrotum. Clin Plast Surg 1988; 15:507–511. - PubMed
-
- Halperin TJ, Slavin SA, Olumi AF, et al. Surgical management of scrotal lymphedema using local flaps. Ann Plast Surg 2007; 59:67–72. - PubMed
-
- Guedes Neto HJ. Surgical treatment of penile-scrotal lymphedema. Lymphology 1996; 29:132–133. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
