

IgE Sensitization Profiles Differ between Adult Patients with Severe and Moderate Atopic Dermatitis
- PMID: 27228091
- PMCID: PMC4881900
- DOI: 10.1371/journal.pone.0156077
IgE Sensitization Profiles Differ between Adult Patients with Severe and Moderate Atopic Dermatitis
Abstract
Background: Atopic dermatitis (AD) is a complex chronic inflammatory disease where allergens can act as specific triggering factors.
Aim: To characterize the specificities of IgE-reactivity in patients with AD to a broad panel of exogenous allergens including microbial and human antigens.
Methodology: Adult patients with AD were grouped according to the SCORAD index, into severe (n = 53) and moderate AD (n = 126). As controls 43 patients were included with seborrhoeic eczema and 97 individuals without history of allergy or skin diseases. Specific IgE reactivity was assessed in plasma using Phadiatop®, ImmunoCap™, micro-arrayed allergens, dot-blotted recombinant Malassezia sympodialis allergens, and immune-blotted microbial and human proteins.
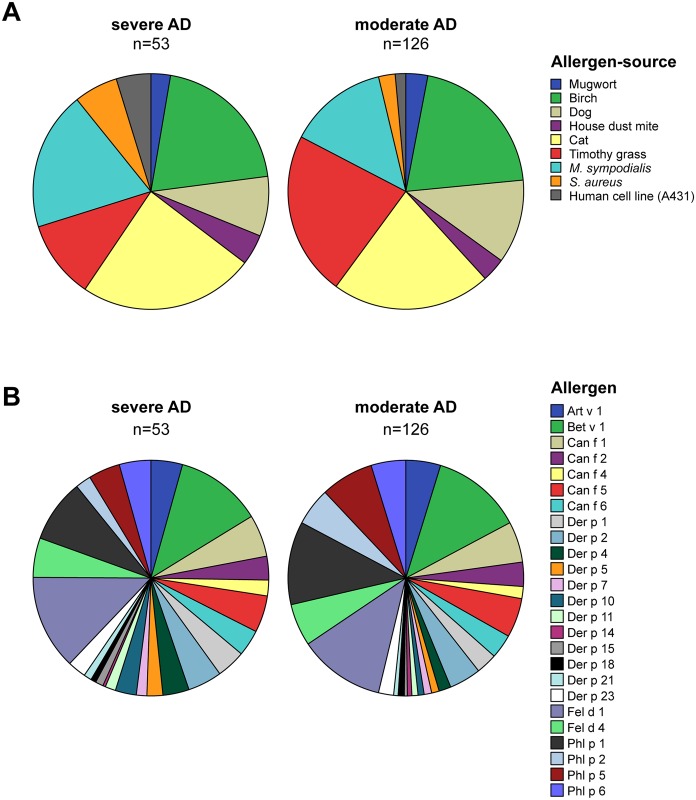
Results: IgE reactivity was detected in 92% of patients with severe and 83% of patients with moderate AD. Sensitization to cat allergens occurred most frequently, followed by sensitization to birch pollen, grass pollen, and to the skin commensal yeast M. sympodialis. Patients with severe AD showed a significantly higher frequency of IgE reactivity to allergens like cat (rFel d 1) and house dust mite (rDer p 4 and 10), to Staphylococcus aureus, M. sympodialis, and to human antigens. In contrast, there were no significant differences in the frequencies of IgE reactivity to the grass pollen allergens rPhl p 1, 2, 5b, and 6 between the two AD groups. Furthermore the IgE reactivity profile of patients with severe AD was more spread towards several different allergen molecules as compared to patients with moderate AD.
Conclusion: We have revealed a hitherto unknown difference regarding the molecular sensitization profile in patients with severe and moderate AD. Molecular profiling towards allergen components may provide a basis for future investigations aiming to explore the environmental, genetic and epigenetic factors which could be responsible for the different appearance and severity of disease phenotypes in AD.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
