

Breast Cancer Risk From Modifiable and Nonmodifiable Risk Factors Among White Women in the United States
- PMID: 27228256
- PMCID: PMC5719876
- DOI: 10.1001/jamaoncol.2016.1025
Breast Cancer Risk From Modifiable and Nonmodifiable Risk Factors Among White Women in the United States
Erratum in
-
Errata.JAMA Oncol. 2016 Oct 1;2(10):1374. doi: 10.1001/jamaoncol.2016.3582. JAMA Oncol. 2016. PMID: 27532671 No abstract available.
Abstract
Importance: An improved model for risk stratification can be useful for guiding public health strategies of breast cancer prevention.
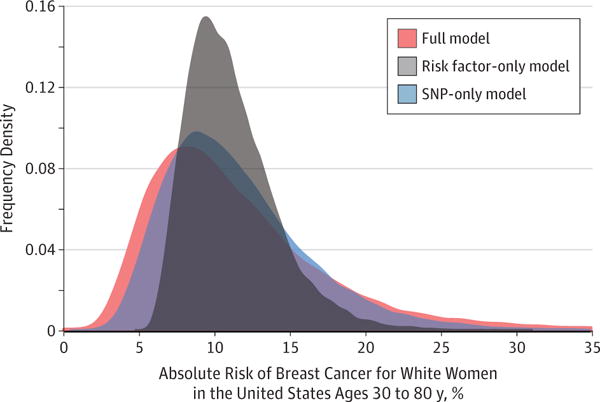
Objective: To evaluate combined risk stratification utility of common low penetrant single nucleotide polymorphisms (SNPs) and epidemiologic risk factors.
Design, setting, and participants: Using a total of 17 171 cases and 19 862 controls sampled from the Breast and Prostate Cancer Cohort Consortium (BPC3) and 5879 women participating in the 2010 National Health Interview Survey, a model for predicting absolute risk of breast cancer was developed combining information on individual level data on epidemiologic risk factors and 24 genotyped SNPs from prospective cohort studies, published estimate of odds ratios for 68 additional SNPs, population incidence rate from the National Cancer Institute-Surveillance, Epidemiology, and End Results Program cancer registry and data on risk factor distribution from nationally representative health survey. The model is used to project the distribution of absolute risk for the population of white women in the United States after adjustment for competing cause of mortality.
Exposures: Single nucleotide polymorphisms, family history, anthropometric factors, menstrual and/or reproductive factors, and lifestyle factors.
Main outcomes and measures: Degree of stratification of absolute risk owing to nonmodifiable (SNPs, family history, height, and some components of menstrual and/or reproductive history) and modifiable factors (body mass index [BMI; calculated as weight in kilograms divided by height in meters squared], menopausal hormone therapy [MHT], alcohol, and smoking).
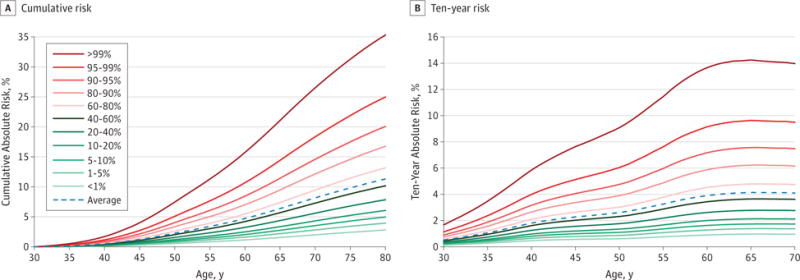
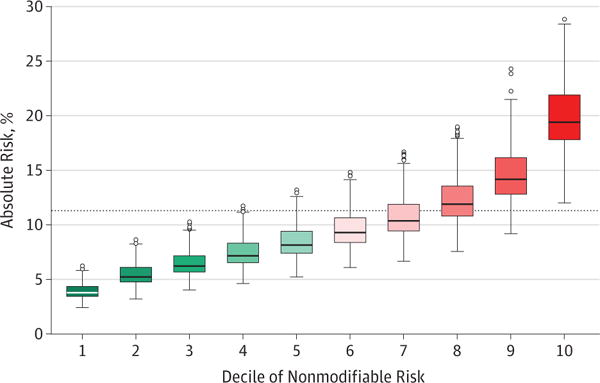
Results: The average absolute risk for a 30-year-old white woman in the United States developing invasive breast cancer by age 80 years is 11.3%. A model that includes all risk factors provided a range of average absolute risk from 4.4% to 23.5% for women in the bottom and top deciles of the risk distribution, respectively. For women who were at the lowest and highest deciles of nonmodifiable risks, the 5th and 95th percentile range of the risk distribution associated with 4 modifiable factors was 2.9% to 5.0% and 15.5% to 25.0%, respectively. For women in the highest decile of risk owing to nonmodifiable factors, those who had low BMI, did not drink or smoke, and did not use MHT had risks comparable to an average woman in the general population.
Conclusions and relevance: This model for absolute risk of breast cancer including SNPs can provide stratification for the population of white women in the United States. The model can also identify subsets of the population at an elevated risk that would benefit most from risk-reduction strategies based on altering modifiable factors. The effectiveness of this model for individual risk communication needs further investigation.
Conflict of interest statement
Figures
Comment in
-
Building and Validating Complex Models of Breast Cancer Risk.JAMA Oncol. 2016 Oct 1;2(10):1271-1272. doi: 10.1001/jamaoncol.2016.0878. JAMA Oncol. 2016. PMID: 27228121 No abstract available.
References
-
- National Cancer Institute. Incident Cases of Breast Cancer in 2014. 2014 http://www.cancer.gov/cancertopics/types/breast/. Accessed October 14, 2014.
-
- Bray F, Ren JS, Masuyer E, Ferlay J. Global estimates of cancer prevalence for 27 sites in the adult population in 2008. Int J Cancer. 2013;132(5):1133–1145. - PubMed
-
- Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359–E386. - PubMed
-
- Madigan MP, Ziegler RG, Benichou J, Byrne C, Hoover RN. Proportion of breast cancer cases in the United States explained by well-established risk factors. J Natl Cancer Inst. 1995;87(22):1681–1685. - PubMed
MeSH terms
Grants and funding
- HHSN268201100001I/HL/NHLBI NIH HHS/United States
- R35 CA197449/CA/NCI NIH HHS/United States
- HHSN268201100004I/HL/NHLBI NIH HHS/United States
- HHSN268201100046C/HL/NHLBI NIH HHS/United States
- HHSN268201100003C/WH/WHI NIH HHS/United States
- U01 CA098216/CA/NCI NIH HHS/United States
- HHSN271201100004C/AG/NIA NIH HHS/United States
- HHSN268201100002C/WH/WHI NIH HHS/United States
- U01 CA098233/CA/NCI NIH HHS/United States
- U01 CA098758/CA/NCI NIH HHS/United States
- HHSN268201100003I/HL/NHLBI NIH HHS/United States
- HHSN268201100002I/HL/NHLBI NIH HHS/United States
- Z01 CP010181/ImNIH/Intramural NIH HHS/United States
- 001/WHO_/World Health Organization/International
- HHSN268201100001C/WH/WHI NIH HHS/United States
- HHSN268201100004C/WH/WHI NIH HHS/United States
- U01 CA098710/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
