

Delirium diagnosis defined by cluster analysis of symptoms versus diagnosis by DSM and ICD criteria: diagnostic accuracy study
- PMID: 27229307
- PMCID: PMC4882791
- DOI: 10.1186/s12888-016-0878-6
Delirium diagnosis defined by cluster analysis of symptoms versus diagnosis by DSM and ICD criteria: diagnostic accuracy study
Abstract
Background: Information on validity and reliability of delirium criteria is necessary for clinicians, researchers, and further developments of DSM or ICD. We compare four DSM and ICD delirium diagnostic criteria versions, which were developed by consensus of experts, with a phenomenology-based natural diagnosis delineated using cluster analysis of delirium features in a sample with a high prevalence of dementia. We also measured inter-rater reliability of each system when applied by two evaluators from distinct disciplines.
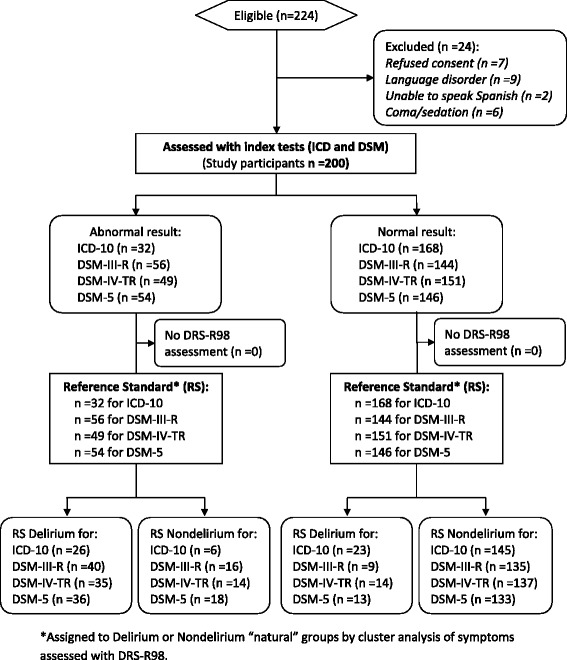
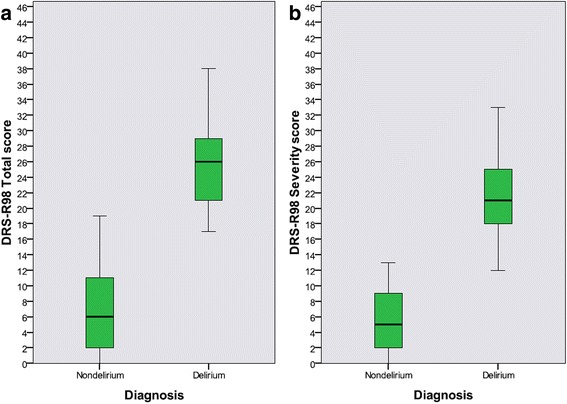
Methods: Cross-sectional analysis of 200 consecutive patients admitted to a skilled nursing facility, independently assessed within 24-48 h after admission with the Delirium Rating Scale-Revised-98 (DRS-R98) and for DSM-III-R, DSM-IV, DSM-5, and ICD-10 criteria for delirium. Cluster analysis (CA) delineated natural delirium and nondelirium reference groups using DRS-R98 items and then diagnostic systems' performance were evaluated against the CA-defined groups using logistic regression and crosstabs for discriminant analysis (sensitivity, specificity, percentage of subjects correctly classified by each diagnostic system and their individual criteria, and performance for each system when excluding each individual criterion are reported). Kappa Index (K) was used to report inter-rater reliability for delirium diagnostic systems and their individual criteria.
Results: 117 (58.5 %) patients had preexisting dementia according to the Informant Questionnaire on Cognitive Decline in the Elderly. CA delineated 49 delirium subjects and 151 nondelirium. Against these CA groups, delirium diagnosis accuracy was highest using DSM-III-R (87.5 %) followed closely by DSM-IV (86.0 %), ICD-10 (85.5 %) and DSM-5 (84.5 %). ICD-10 had the highest specificity (96.0 %) but lowest sensitivity (53.1 %). DSM-III-R had the best sensitivity (81.6 %) and the best sensitivity-specificity balance. DSM-5 had the highest inter-rater reliability (K =0.73) while DSM-III-R criteria were the least reliable.
Conclusions: Using our CA-defined, phenomenologically-based delirium designations as the reference standard, we found performance discordance among four diagnostic systems when tested in subjects where comorbid dementia was prevalent. The most complex diagnostic systems have higher accuracy and the newer DSM-5 have higher reliability. Our novel phenomenological approach to designing a delirium reference standard may be preferred to guide revisions of diagnostic systems in the future.
Keywords: Cluster analysis; Delirium; Delirium rating scale-revised-98; Dementia; Diagnostic and statistical manual of mental disorders; Discriminant analysis; International classification of diseases; Reliability; Sensitivity and specificity.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
