

The next generation of therapeutics for chronic kidney disease
- PMID: 27230798
- PMCID: PMC5511522
- DOI: 10.1038/nrd.2016.67
The next generation of therapeutics for chronic kidney disease
Abstract
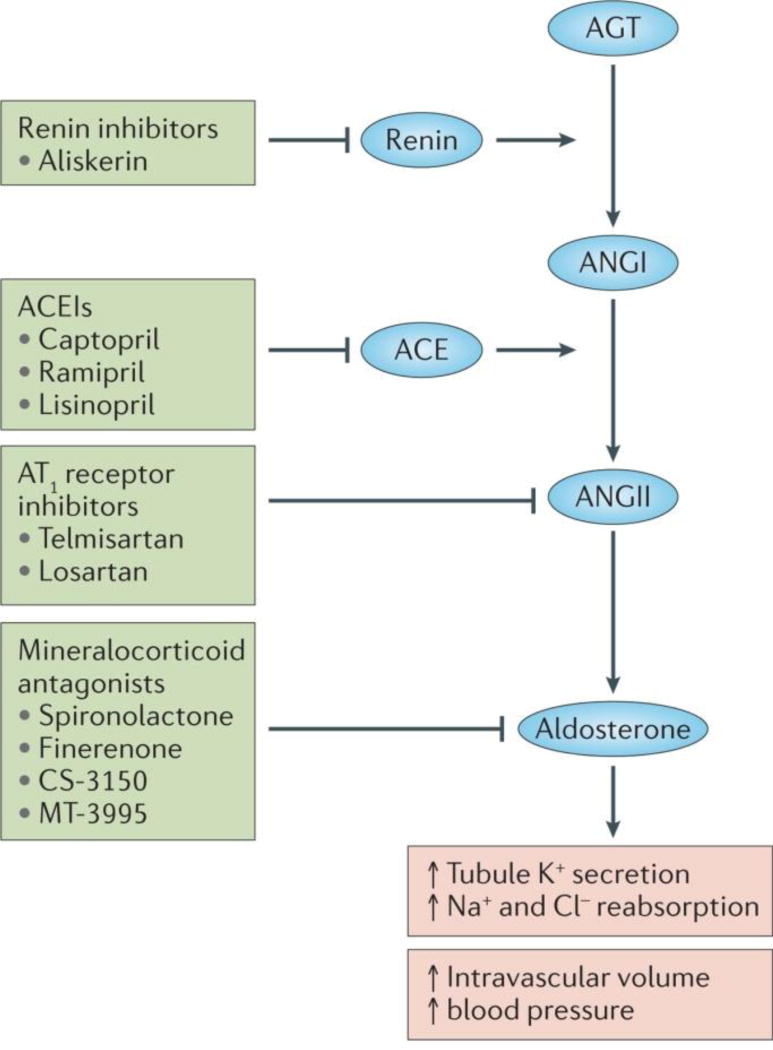
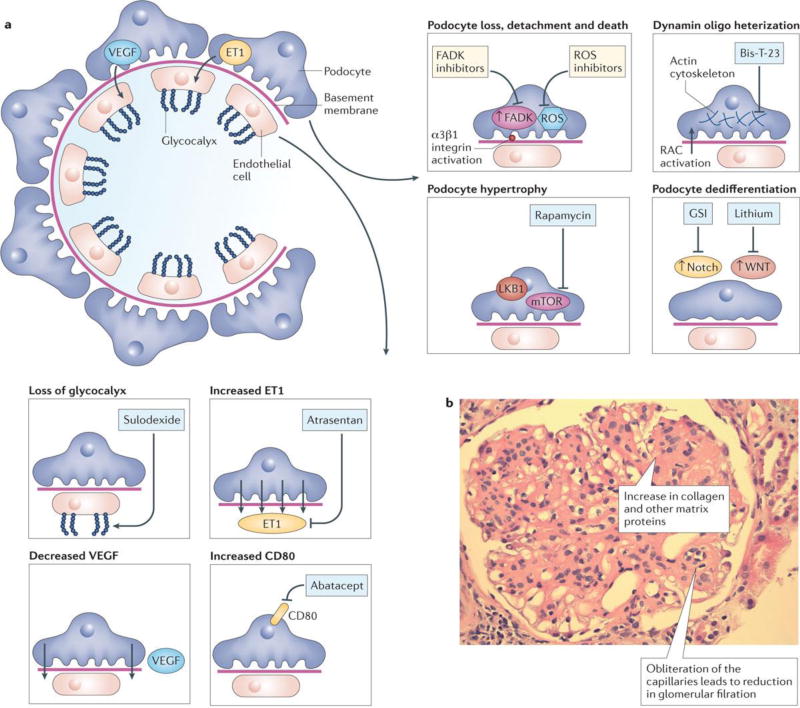
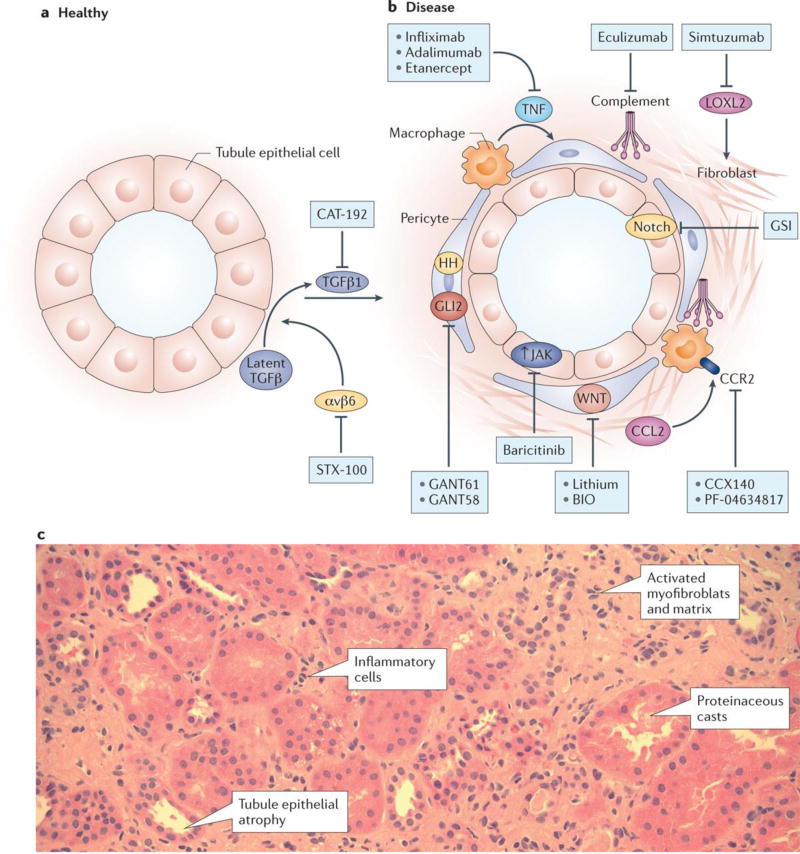
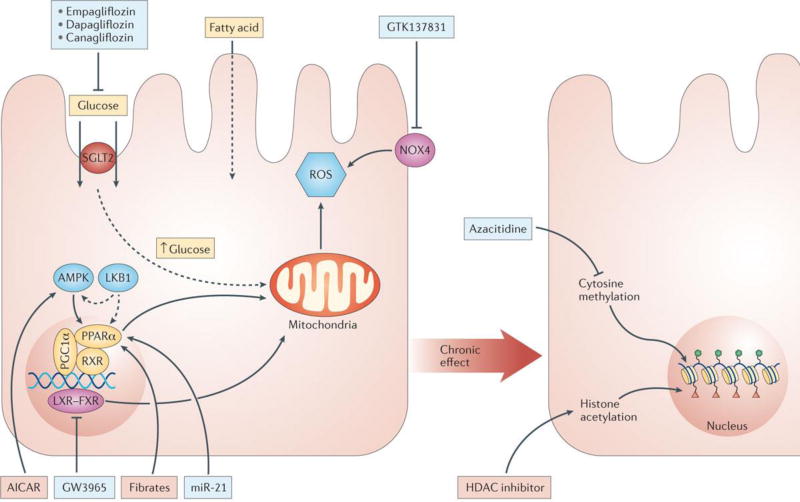
Chronic kidney disease (CKD) represents a leading cause of death in the United States. There is no cure for this disease, with current treatment strategies relying on blood pressure control through blockade of the renin-angiotensin system. Such approaches only delay the development of end-stage kidney disease and can be associated with serious side effects. Recent identification of several novel mechanisms contributing to CKD development - including vascular changes, loss of podocytes and renal epithelial cells, matrix deposition, inflammation and metabolic dysregulation - has revealed new potential therapeutic approaches for CKD. This Review assesses emerging strategies and agents for CKD treatment, highlighting the associated challenges in their clinical development.
Figures
References
-
- Foley RN, Collins AJ. The USRDS: what you need to know about what it can and can't tell us about ESRD. Clinical journal of the American Society of Nephrology : CJASN. 2013;8:845–851. - PubMed
-
- Weiner DE, et al. Kidney function and risk of cardiovascular disease and mortality in kidney transplant recipients: the FAVORIT trial. American journal of transplantation : official journal of the American Society of Transplantation and the American Society of Transplant Surgeons. 2012;12:2437–2445. - PMC - PubMed
-
- Herzog CA, et al. Cardiovascular disease in chronic kidney disease. A clinical update from Kidney Disease: Improving Global Outcomes (KDIGO) Kidney international. 2011;80:572–586. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
