

Mosaic Loss of Chromosome Y in Blood Is Associated with Alzheimer Disease
- PMID: 27231129
- PMCID: PMC4908225
- DOI: 10.1016/j.ajhg.2016.05.014
Mosaic Loss of Chromosome Y in Blood Is Associated with Alzheimer Disease
Abstract
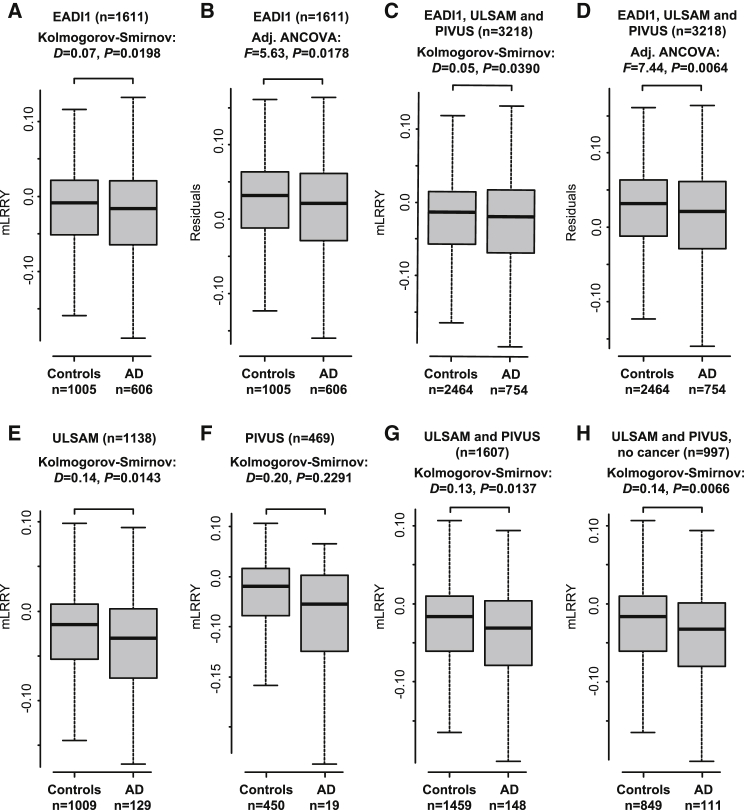
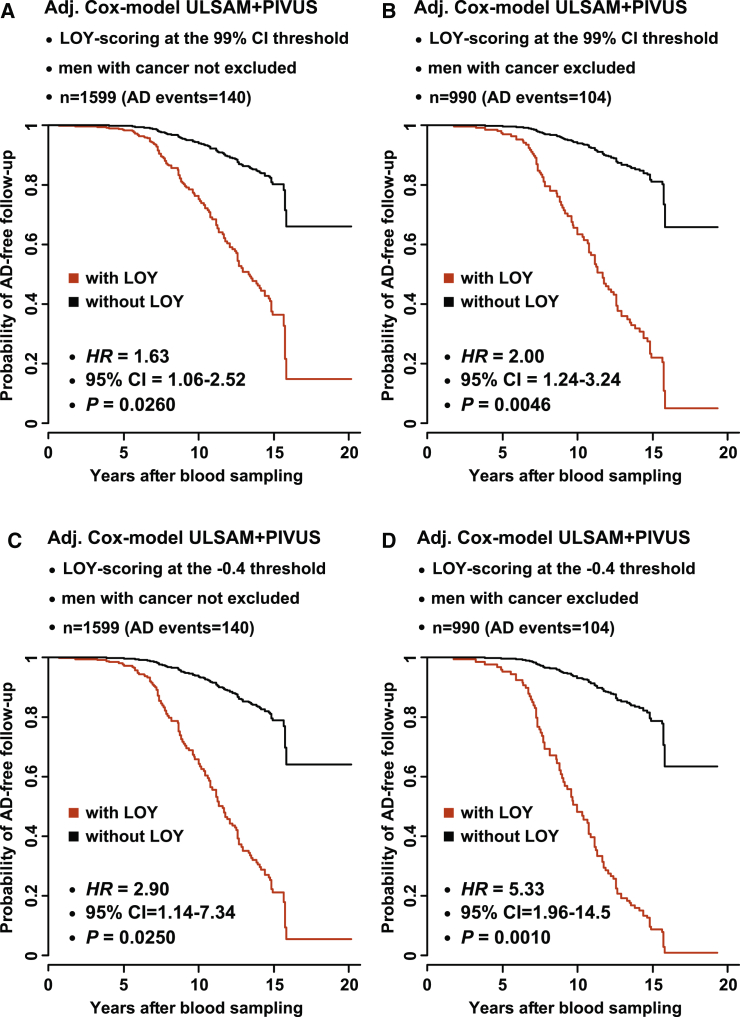
Men have a shorter life expectancy compared with women but the underlying factor(s) are not clear. Late-onset, sporadic Alzheimer disease (AD) is a common and lethal neurodegenerative disorder and many germline inherited variants have been found to influence the risk of developing AD. Our previous results show that a fundamentally different genetic variant, i.e., lifetime-acquired loss of chromosome Y (LOY) in blood cells, is associated with all-cause mortality and an increased risk of non-hematological tumors and that LOY could be induced by tobacco smoking. We tested here a hypothesis that men with LOY are more susceptible to AD and show that LOY is associated with AD in three independent studies of different types. In a case-control study, males with AD diagnosis had higher degree of LOY mosaicism (adjusted odds ratio = 2.80, p = 0.0184, AD events = 606). Furthermore, in two prospective studies, men with LOY at blood sampling had greater risk for incident AD diagnosis during follow-up time (hazard ratio [HR] = 6.80, 95% confidence interval [95% CI] = 2.16-21.43, AD events = 140, p = 0.0011). Thus, LOY in blood is associated with risks of both AD and cancer, suggesting a role of LOY in blood cells on disease processes in other tissues, possibly via defective immunosurveillance. As a male-specific risk factor, LOY might explain why males on average live shorter lives than females.
Copyright © 2016 The Author(s). Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Bettens K., Sleegers K., Van Broeckhoven C. Genetic insights in Alzheimer’s disease. Lancet Neurol. 2013;12:92–104. - PubMed
-
- Hardy J., Selkoe D.J. The amyloid hypothesis of Alzheimer’s disease: progress and problems on the road to therapeutics. Science. 2002;297:353–356. - PubMed
-
- Gatz M., Reynolds C.A., Fratiglioni L., Johansson B., Mortimer J.A., Berg S., Fiske A., Pedersen N.L. Role of genes and environments for explaining Alzheimer disease. Arch. Gen. Psychiatry. 2006;63:168–174. - PubMed
-
- Lambert J.C., Ibrahim-Verbaas C.A., Harold D., Naj A.C., Sims R., Bellenguez C., DeStafano A.L., Bis J.C., Beecham G.W., Grenier-Boley B., European Alzheimer’s Disease Initiative (EADI) Genetic and Environmental Risk in Alzheimer’s Disease. Alzheimer’s Disease Genetic Consortium. Cohorts for Heart and Aging Research in Genomic Epidemiology Meta-analysis of 74,046 individuals identifies 11 new susceptibility loci for Alzheimer’s disease. Nat. Genet. 2013;45:1452–1458. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
