

Enhanced volumetric visualization for real time 4D intraoperative ophthalmic swept-source OCT
- PMID: 27231623
- PMCID: PMC4871083
- DOI: 10.1364/BOE.7.001815
Enhanced volumetric visualization for real time 4D intraoperative ophthalmic swept-source OCT
Abstract
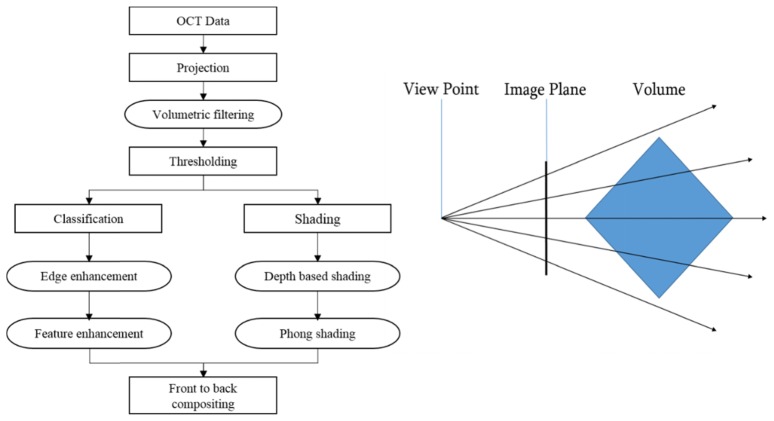
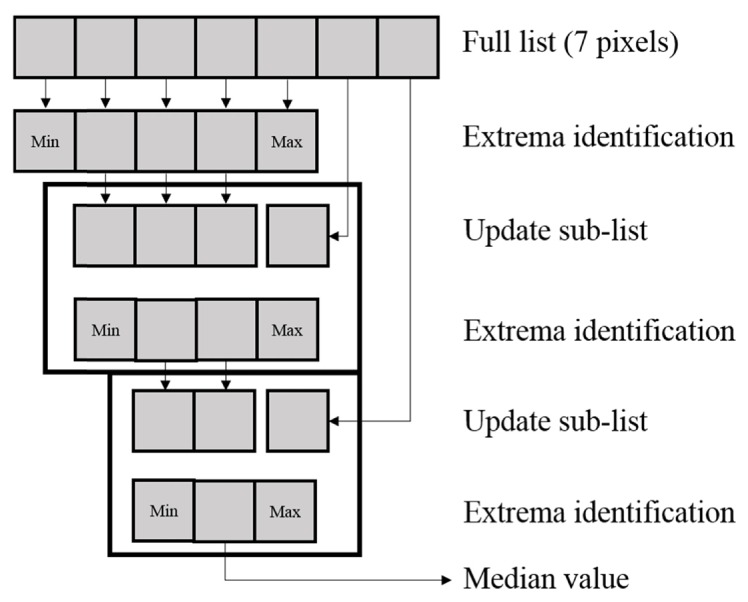
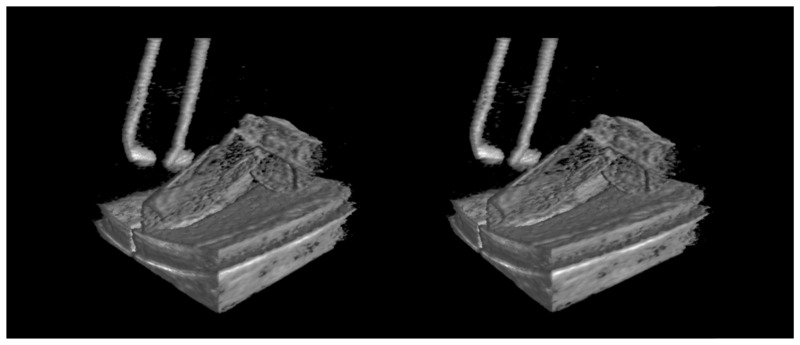
Current-generation software for rendering volumetric OCT data sets based on ray casting results in volume visualizations with indistinct tissue features and sub-optimal depth perception. Recent developments in hand-held and microscope-integrated intrasurgical OCT designed for real-time volumetric imaging motivate development of rendering algorithms which are both visually appealing and fast enough to support real time rendering, potentially from multiple viewpoints for stereoscopic visualization. We report on an enhanced, real time, integrated volumetric rendering pipeline which incorporates high performance volumetric median and Gaussian filtering, boundary and feature enhancement, depth encoding, and lighting into a ray casting volume rendering model. We demonstrate this improved model implemented on graphics processing unit (GPU) hardware for real-time volumetric rendering of OCT data during tissue phantom and live human surgical imaging. We show that this rendering produces enhanced 3D visualizations of pathology and intraoperative maneuvers compared to standard ray casting.
Keywords: (100.0100) Image processing; (110.4500) Optical coherence tomography; (170.4460) Ophthalmic optics and devices.
Figures







Similar articles
-
Processing-Aware Real-Time Rendering for Optimized Tissue Visualization in Intraoperative 4D OCT.Med Image Comput Comput Assist Interv. 2020 Oct;12265:267-276. doi: 10.1007/978-3-030-59722-1_26. Epub 2020 Sep 29. Med Image Comput Comput Assist Interv. 2020. PMID: 34085059 Free PMC article.
-
Surgical microscope integrated MHz SS-OCT with live volumetric visualization.Biomed Opt Express. 2023 Jan 23;14(2):846-865. doi: 10.1364/BOE.477386. eCollection 2023 Feb 1. Biomed Opt Express. 2023. PMID: 36874504 Free PMC article.
-
Real-time 4D signal processing and visualization using graphics processing unit on a regular nonlinear-k Fourier-domain OCT system.Opt Express. 2010 May 24;18(11):11772-84. doi: 10.1364/OE.18.011772. Opt Express. 2010. PMID: 20589038 Free PMC article.
-
State-of-the-art retinal optical coherence tomography.Prog Retin Eye Res. 2008 Jan;27(1):45-88. doi: 10.1016/j.preteyeres.2007.07.005. Epub 2007 Aug 11. Prog Retin Eye Res. 2008. PMID: 18036865 Review.
-
Optical Coherence Tomography for Retinal Surgery: Perioperative Analysis to Real-Time Four-Dimensional Image-Guided Surgery.Invest Ophthalmol Vis Sci. 2016 Jul 1;57(9):OCT37-50. doi: 10.1167/iovs.16-19277. Invest Ophthalmol Vis Sci. 2016. PMID: 27409495 Free PMC article. Review.
Cited by
-
Novel microscope-integrated stereoscopic heads-up display for intrasurgical optical coherence tomography.Biomed Opt Express. 2016 Apr 6;7(5):1711-26. doi: 10.1364/BOE.7.001711. eCollection 2016 May 1. Biomed Opt Express. 2016. PMID: 27231616 Free PMC article.
-
Three-dimensional pattern of extraretinal neovascular development in retinopathy of prematurity.Graefes Arch Clin Exp Ophthalmol. 2019 Apr;257(4):677-688. doi: 10.1007/s00417-019-04274-6. Epub 2019 Feb 21. Graefes Arch Clin Exp Ophthalmol. 2019. PMID: 30790072 Free PMC article.
-
Visualization of surgical maneuvers using intraoperative real-time volumetric optical coherence tomography.Biomed Opt Express. 2023 Jun 29;14(7):3798-3811. doi: 10.1364/BOE.488967. eCollection 2023 Jul 1. Biomed Opt Express. 2023. PMID: 37497507 Free PMC article.
-
Review of intraoperative optical coherence tomography: technology and applications [Invited].Biomed Opt Express. 2017 Feb 21;8(3):1607-1637. doi: 10.1364/BOE.8.001607. eCollection 2017 Mar 1. Biomed Opt Express. 2017. PMID: 28663853 Free PMC article.
-
Intraocular Pressure and Big Bubble Diameter in Deep Anterior Lamellar Keratoplasty: An Ex-Vivo Microscope-Integrated OCT With Heads-Up Display Study.Asia Pac J Ophthalmol (Phila). 2017 Sep-Oct;6(5):412-417. doi: 10.22608/APO.2017265. Asia Pac J Ophthalmol (Phila). 2017. PMID: 28930381 Free PMC article.
References
-
- Lee L. B., Srivastava S. K., “Intraoperative spectral-domain optical coherence tomography during complex retinal detachment repair,” Ophthalmic Surg. Lasers Imaging 42, e71–e74 (2011). - PubMed
-
- Lankenau E., Klinger D., Winter C., Malik A., Müller H. H., Oelckers S., Pau H.-W., Just T., Hüttmann G., “Combining optical coherence tomography (OCT) with an operating microscope,” in Advances in Medical Engineering (Springer, 2007), pp. 343–348.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical