

Immunologic profiles of multiple sclerosis treatments reveal shared early B cell alterations
- PMID: 27231713
- PMCID: PMC4872020
- DOI: 10.1212/NXI.0000000000000240
Immunologic profiles of multiple sclerosis treatments reveal shared early B cell alterations
Abstract
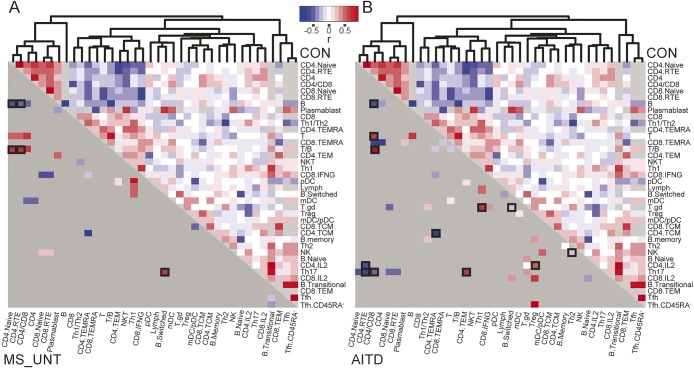
Objective: We undertook a systems immunology approach of the adaptive immune system in multiple sclerosis (MS), overcoming tradeoffs between scale and level of detail, in order to identify the immunologic signature of MS and the changes wrought by current immunomodulatory treatments.
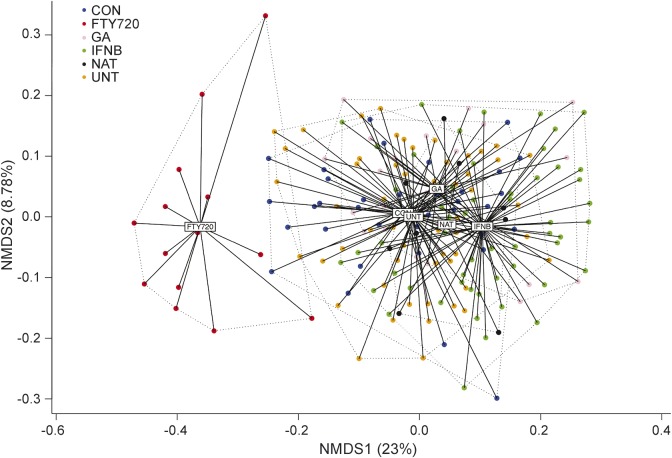
Methods: We developed a comprehensive flow cytometry platform measuring 38 immunologic cell types in the peripheral blood of 245 individuals in a routine clinical setting. These include patients with MS, untreated or receiving any of 4 current immunomodulatory treatments (interferon-β, glatiramer acetate, natalizumab, or fingolimod), patients with autoimmune thyroid disease, and healthy controls.
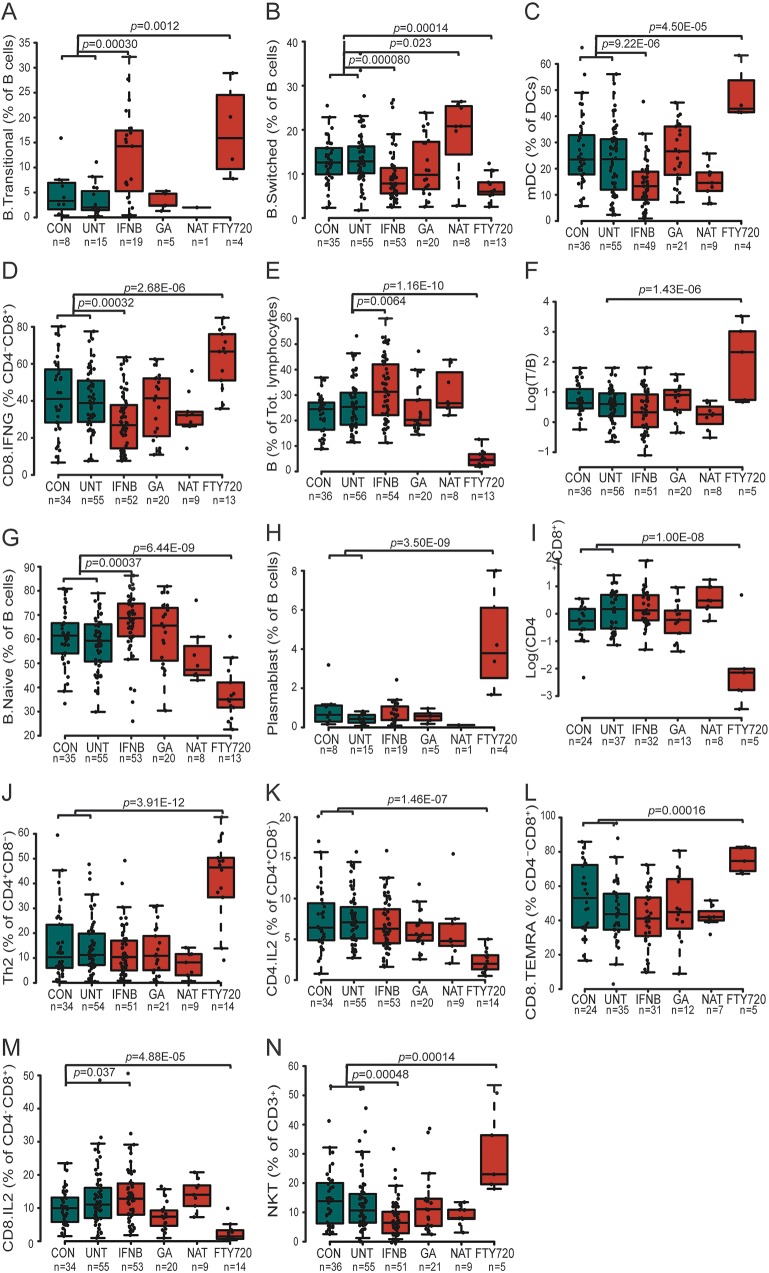
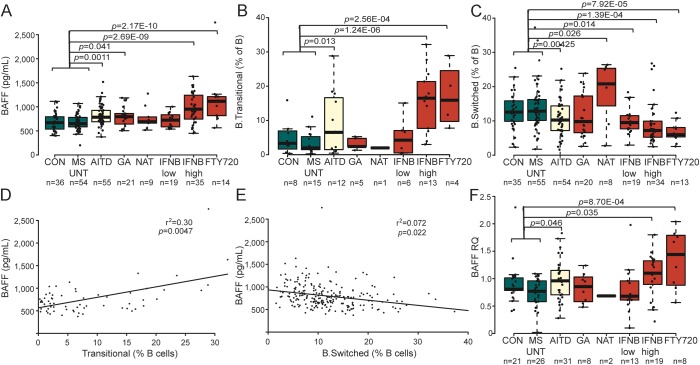
Results: An increase in memory CD8(+) T cells and B cells was observed in untreated patients with MS. Interferon-β and fingolimod induce significant changes upon multiple aspects of the peripheral immune system, with an unexpectedly prominent alteration of B cells. Overall, both treatments push the immune system in different directions, with only 2 significant effects shared across these treatments-an increase in transitional B cells and a decrease in class-switched B cells. We further identified heightened B cell-activating factor (BAFF) levels as regulating this shared B cell pathway.
Conclusions: A systems immunology approach established different immunologic profiles induced by current immunomodulatory MS treatments, offering perspectives for personalized medicine. Pathways shared between the immunologic architecture of existing efficacious treatments identify targets for future treatment design.
Figures

References
-
- Roep BO, Buckner J, Sawcer S, Toes R, Zipp F. The problems and promises of research into human immunology and autoimmune disease. Nat Med 2012;18:48–53. - PubMed
-
- Linker RA, Kieseier BC, Gold R. Identification and development of new therapeutics for multiple sclerosis. Trends Pharmacol Sci 2008;29:558–565. - PubMed
-
- Hauser SL, Chan JR, Oksenberg JR. Multiple sclerosis: prospects and promise. Ann Neurol 2013;74:317–327. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials