

The Electronic CardioMetabolic Program (eCMP) for Patients With Cardiometabolic Risk: A Randomized Controlled Trial
- PMID: 27234480
- PMCID: PMC4902854
- DOI: 10.2196/jmir.5143
The Electronic CardioMetabolic Program (eCMP) for Patients With Cardiometabolic Risk: A Randomized Controlled Trial
Abstract
Background: Effective lifestyle interventions targeting high-risk adults that are both practical for use in ambulatory care settings and scalable at a population management level are needed.
Objective: Our aim was to examine the potential effectiveness, feasibility, and acceptability of delivering an evidence-based Electronic Cardio-Metabolic Program (eCMP) for improving health-related quality of life, improving health behaviors, and reducing cardiometabolic risk factors in ambulatory care high-risk adults.
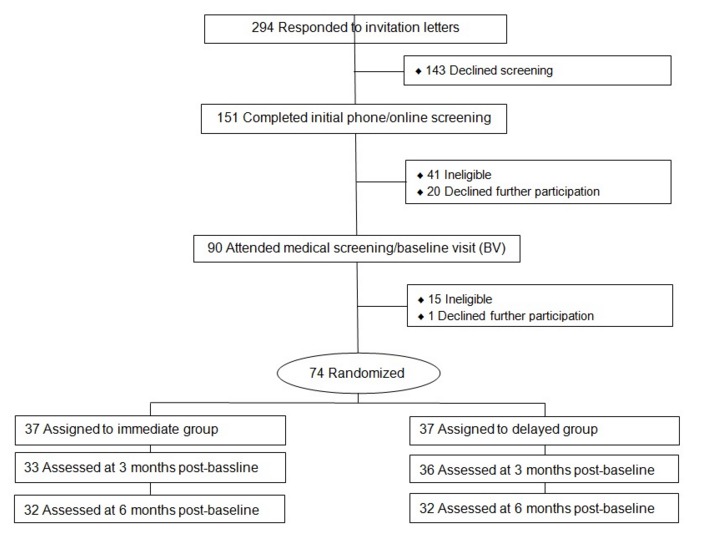
Methods: We conducted a randomized, wait-list controlled trial with 74 adults aged ≥18 years recruited from a large multispecialty health care organization. Inclusion criteria were (1) BMI ≥35 kg/m(2) and prediabetes, previous gestational diabetes and/or metabolic syndrome, or (2) BMI ≥30 kg/m(2) and type 2 diabetes and/or cardiovascular disease. Participants had a mean age of 59.7 years (SD 11.2), BMI 37.1 kg/m(2) (SD 5.4) and were 59.5% female, 82.4% white. Participants were randomized to participate in eCMP immediately (n=37) or 3 months later (n=37). eCMP is a 6-month program utilizing video conferencing, online tools, and pre-recorded didactic videos to deliver evidence-based curricula. Blinded outcome assessments were conducted at 3 and 6 months postbaseline. Data were collected and analyzed between 2014 and 2015. The primary outcome was health-related quality of life. Secondary outcomes included biometric cardiometabolic risk factors (eg, body weight), self-reported diet and physical activity, mental health status, retention, session attendance, and participant satisfaction.
Results: Change in quality of life was not significant in both immediate and delayed participants. Both groups significantly lost weight and reduced waist circumference at 6 months, with some cardiometabolic factors trending accordingly. Significant reduction in self-reported anxiety and perceived stress was seen in the immediate intervention group at 6 months. Retention rate was 93% at 3 months and 86% at 6 months post-baseline. Overall eCMP attendance was high with 59.5-83.8% of immediate and delayed intervention participants attending 50% of the virtual stress management and behavioral lifestyle sessions and 37.8-62.2% attending at least 4 out of 7 in-person physical activity sessions. The intervention received high ratings for satisfaction.
Conclusions: The technology-assisted eCMP is a feasible and well-accepted intervention and may significantly decrease cardiometabolic risk among high-risk individuals.
Trial registration: Clinicaltrials.gov NCT02246400; https://clinicaltrials.gov/ct2/show/NCT02246400 (Archived by WebCite at http://www.webcitation.org/6h6mWWokP).
Keywords: behavior change; cardiovascular disease; health technology; lifestyle; metabolic syndrome; prevention.
Conflict of interest statement
Conflicts of Interest: None declared.
References
-
- Jensen MD, Ryan DH, Apovian CM, Ard JD, Comuzzie AG, Donato KA, Hu FB, Hubbard VS, Jakicic JM, Kushner RF, Loria CM, Millen BE, Nonas CA, Pi-Sunyer FX, Stevens J, Stevens VJ, Wadden TA, Wolfe BM, Yanovski SZ, American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Obesity S. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. J Am Coll Cardiol. 2014 Jul 1;63(25 Pt B):2985–3023. doi: 10.1016/j.jacc.2013.11.004. http://linkinghub.elsevier.com/retrieve/pii/S0735-1097(13)06030-0 S0735-1097(13)06030-0 - DOI - PubMed
-
- Spring B, Duncan JM, Janke EA, Kozak AT, McFadden HG, DeMott A, Pictor A, Epstein LH, Siddique J, Pellegrini CA, Buscemi J, Hedeker D. Integrating technology into standard weight loss treatment: a randomized controlled trial. JAMA Intern Med. 2013 Jan 28;173(2):105–111. doi: 10.1001/jamainternmed.2013.1221. http://europepmc.org/abstract/MED/23229890 1485082 - DOI - PMC - PubMed
-
- Cole-Lewis H, Kershaw T. Text messaging as a tool for behavior change in disease prevention and management. Epidemiol Rev. 2010;32:56–69. doi: 10.1093/epirev/mxq004. http://europepmc.org/abstract/MED/20354039 mxq004 - DOI - PMC - PubMed
-
- Chaudhry B, Wang J, Wu S, Maglione M, Mojica W, Roth E, Morton SC, Shekelle PG. Systematic review: impact of health information technology on quality, efficiency, and costs of medical care. Ann Intern Med. 2006 May 16;144(10):742–752.0000605-200605160-00125 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
