

De Novo vs Nevus-Associated Melanomas: Differences in Associations With Prognostic Indicators and Survival
- PMID: 27235387
- PMCID: PMC5939856
- DOI: 10.1093/jnci/djw121
De Novo vs Nevus-Associated Melanomas: Differences in Associations With Prognostic Indicators and Survival
Abstract
Background: Although 20% to 30% of melanomas are histopathologically 'nevus associated,' the majority of melanomas arise de novo, ie, in clinically normal skin with no associated nevus. We examined whether these forms of melanoma differed in their associations with clinical and histopathologic features and patient survival.
Methods: We analyzed two prospective cohorts from our institution with protocol-driven follow-up information (NYU1, n = 1024; NYU2, n = 1125). We used univariate and multivariable analyses to examine associations between de novo vs nevus-associated melanoma classification and age, anatomic site, tumor thickness, tumor ulceration, mitotic index, histological subtype, clinical stage, and survival. We tested the associations identified in NYU1 using NYU2 as a replication cohort. All tests of statistical significance were two-sided.
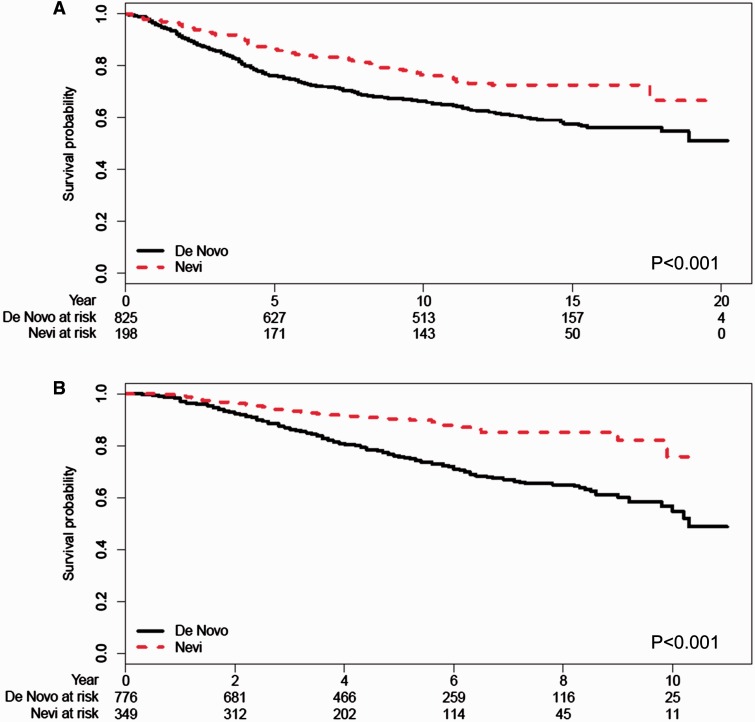
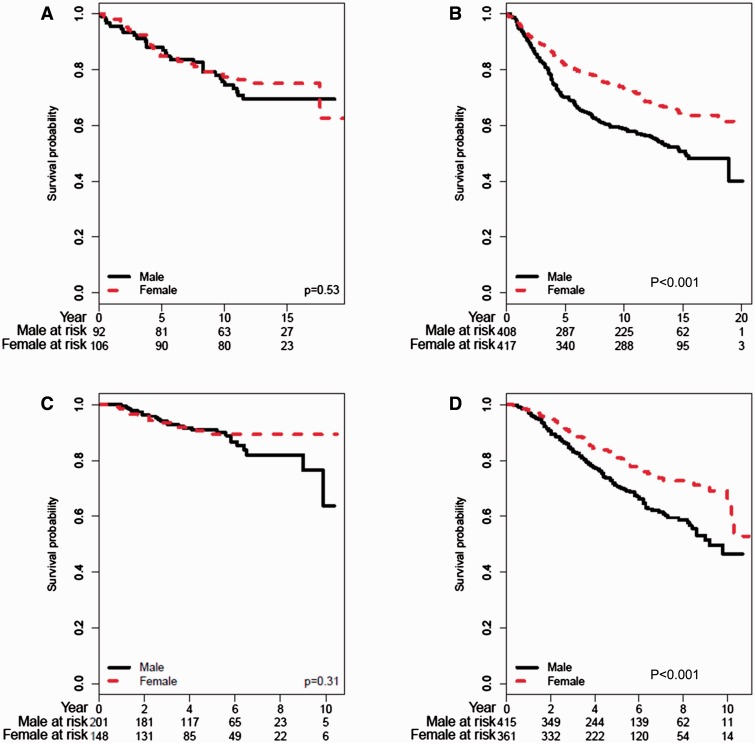
Results: In NYU1, de novo melanomas were associated with tumor thickness greater than 1.0 mm (odds ratio [OR] = 1.96, 95% confidence interval [CI] = 1.43 to 2.70, P < .001), ulceration (OR = 1.65, 95% CI = 1.10 to 2.54, P = .02), nodular subtype (OR = 3.26, 95% CI = 1.70 to 7.11, P = .001), greater than stage I (OR = 2.35, 95% CI = 1.65 to 3.40, P < .001), older age (OR = 1.64, 95% CI = 1.18 to 2.30, P = .004), and shorter overall survival (HR = 1.63, 95% CI = 1.22 to 2.18, P < .001). In NYU2, de novo melanoma was again statistically significantly associated with thickness greater than 1.0 mm (OR = 2.24, 95% CI = 1.72 to 2.93, P < .001), ulceration (OR = 2.88, 95% CI = 1.95 to 4.37, P < .001), nodular subtype (OR = 2.41, 95% CI = 1.75 to 3.37, P < .001), greater than stage I (OR = 2.42, 95% CI = 1.80 to 3.29, P < .001), older age (OR = 1.68, 95% CI = 1.31 to 2.17, P < .001), and shorter overall survival (HR = 2.52, 95% CI = 1.78 to 3.56, P < .001). In multivariable analysis, de novo classification was an independent, poor prognostic indicator in NYU2 (HR = 1.70, 95% CI = 1.19 to 2.44, P = .004). Male patients had a statistically significantly worse survival than female patients if their melanoma was de novo (NYU1, P < .001; NYU2, P < .001); unexpectedly, there was no sex difference in survival among patients with nevus-associated tumors.
Conclusions: These data suggest that de novo melanomas are more aggressive than nevus-associated melanomas. This classification scheme may also provide a useful framework for investigations into sex differences in melanoma outcomes.
© The Author 2016. Published by Oxford University Press. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Stolz W, Schmoeckel C, Landthaler M , et al. . Association of early malignant melanoma with nevocytic nevi . Cancer. 1989. ; 63 ( 3 ): 550 - 555 . - PubMed
-
- Black WC. Residual dysplastic and other nevi in superficial spreading melanoma. Clinical correlations and association with sun damage . Cancer. 1988. ; 62 ( 1 ): 163 - 173 . - PubMed
-
- Clark WH, Jr, Elder DE, Guerry Dt , et al. . A study of tumor progression: the precursor lesions of superficial spreading and nodular melanoma . Hum Pathol. 1984. ; 15 ( 12 ): 1147 - 1165 . - PubMed
-
- Cook MG, Robertson I. Melanocytic dysplasia and melanoma . Histopathology. 1985. ; 9 ( 6 ): 647 - 658 . - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
