

Imaging right ventricular function to predict outcome in pulmonary arterial hypertension
- PMID: 27236116
- PMCID: PMC5001160
- DOI: 10.1016/j.ijcard.2016.05.015
Imaging right ventricular function to predict outcome in pulmonary arterial hypertension
Abstract
Background: Right ventricular (RV) function is a major determinant of outcome in pulmonary arterial hypertension (PAH). However, uncertainty persists about the optimal method of evaluation.
Methods: We measured RV end-systolic and end-diastolic volumes (ESV and EDV) using cardiac magnetic resonance imaging and RV pressures during right heart catheterization in 140 incident PAH patients and 22 controls. A maximum RV pressure (Pmax) was calculated from the nonlinear extrapolations of early and late systolic portions of the RV pressure curve. The gold standard measure of RV function adaptation to afterload, or RV-arterial coupling (Ees/Ea) was estimated by the stroke volume (SV)/ESV ratio (volume method) or as Pmax/mean pulmonary artery pressure (mPAP) minus 1 (pressure method) (n=84). RV function was also assessed by ejection fraction (EF), right atrial pressure (RAP) and SV.
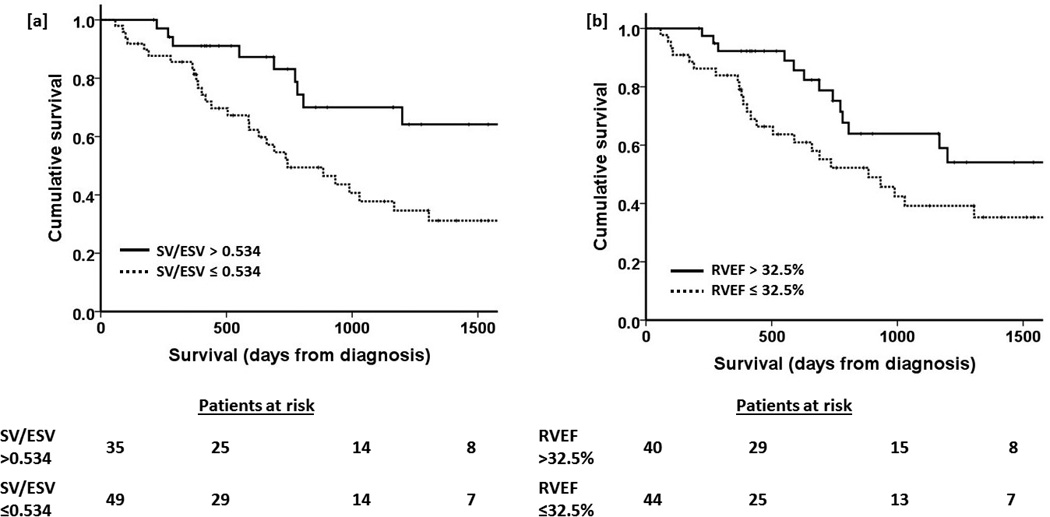
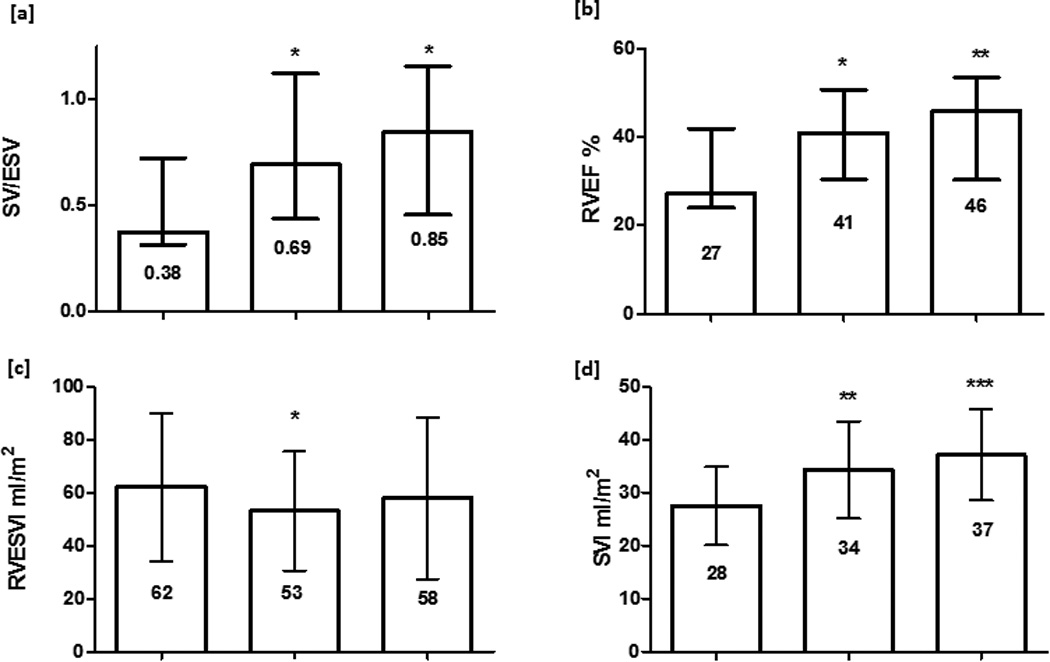
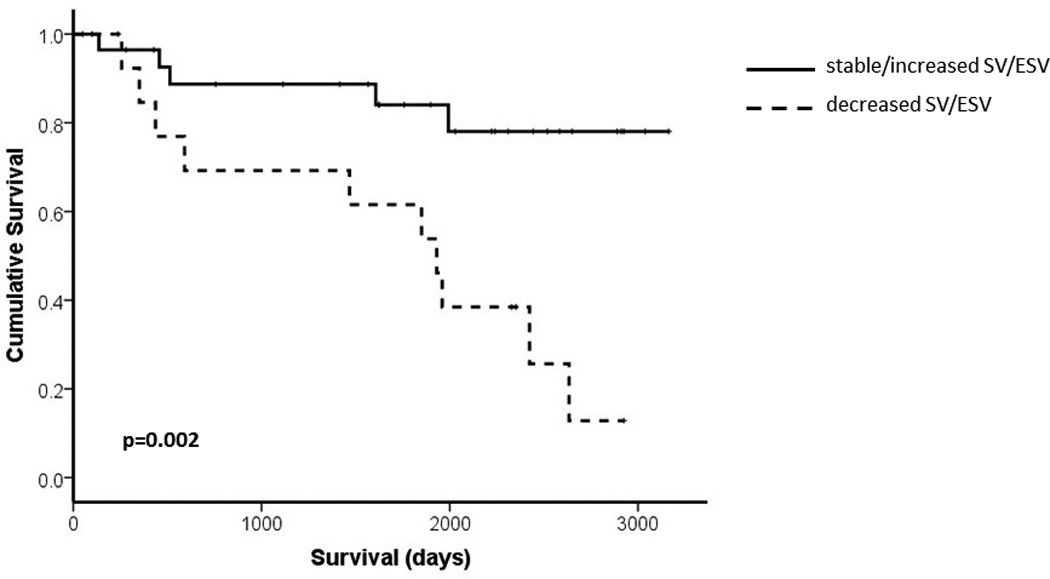
Results: Higher Ea and RAP, and lower compliance, SV and EF predicted outcome at univariate analysis. Ees/Ea estimated by the pressure method did not predict outcome but Ees/Ea estimated by the volume method (SV/ESV) did. At multivariate analysis, only SV/ESV and EF were independent predictors of outcome. Survival was poorer in patients with a fall in EF or SV/ESV during follow-up (n=44, p=0.008).
Conclusion: RV function to predict outcome in PAH is best evaluated by imaging derived SV/ESV or EF. In this study, there was no added value of invasive measurements or simplified pressure-derived estimates of RV-arterial coupling.
Keywords: Pressure–volume relationship; Prognosis; Pulmonary hypertension; Right ventricular dysfunction.
Copyright © 2016 Elsevier Ireland Ltd. All rights reserved.
Conflict of interest statement
Dr Bellofiore, Dr Vanderpool, Dr Chesler and Professor Naeije report no relationships that could be construed as a conflict of interest.
Figures
References
-
- Vonk-Noordegraaf A, Haddad F, Chin KM, Forfia PR, Kawut SM, Lumens J, Naeije R, Newman J, Oudiz RJ, Provencher S, Torbicki A, Voelkel NF, Hassoun PM. Right heart adaptation to pulmonary arterial hypertension: physiology and pathobiology. J Am Coll Cardiol. 2013;62(25 Suppl):D22–D33. - PubMed
-
- Naeije R. Assessment of right ventricular function in pulmonary hypertension. Curr Hypertens Rep. 2015;17(5):35. - PubMed
-
- Maughan WL, Shoukas AA, Sagawa K, Weisfeldt ML. Instantaneous pressure-volume relationship of the canine right ventricle. Circ Res. 1979;44(3):309–315. - PubMed
-
- Brimioulle S, Wauthy P, Ewalenko P, Rondelet Bt, Vermeulen F, Kerbaul F, Naeije R. Single-beat estimation of right ventricular end-systolic pressure-volume relationship. American Journal of Physiology - Heart and Circulatory Physiology. 2003;284(5):H1625–H1630. - PubMed
-
- Sanz J, Garcia-Alvarez A, Fernandez-Friera L, Nair A, Mirelis JG, Sawit ST, Pinney S, Fuster V. Right ventriculo-arterial coupling in pulmonary hypertension: a magnetic resonance study. Heart. 2012;98:238–243. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
