

Strength of Validation for Surrogate End Points Used in the US Food and Drug Administration's Approval of Oncology Drugs
- PMID: 27236424
- PMCID: PMC5104665
- DOI: 10.1016/j.mayocp.2016.02.012
Strength of Validation for Surrogate End Points Used in the US Food and Drug Administration's Approval of Oncology Drugs
Abstract
Objective: To determine the strength of the surrogate-survival correlation for cancer drug approvals based on a surrogate.
Participants and methods: We performed a retrospective study of the US Food and Drug Administration (FDA) database, with focused searches of MEDLINE and Google Scholar. Among cancer drugs approved based on a surrogate end point, we examined previous publications assessing the strength of the surrogate-survival correlation. Specifically, we identified the percentage of surrogate approvals lacking any formal analysis of the strength of the surrogate-survival correlation, and when conducted, the strength of such correlations.
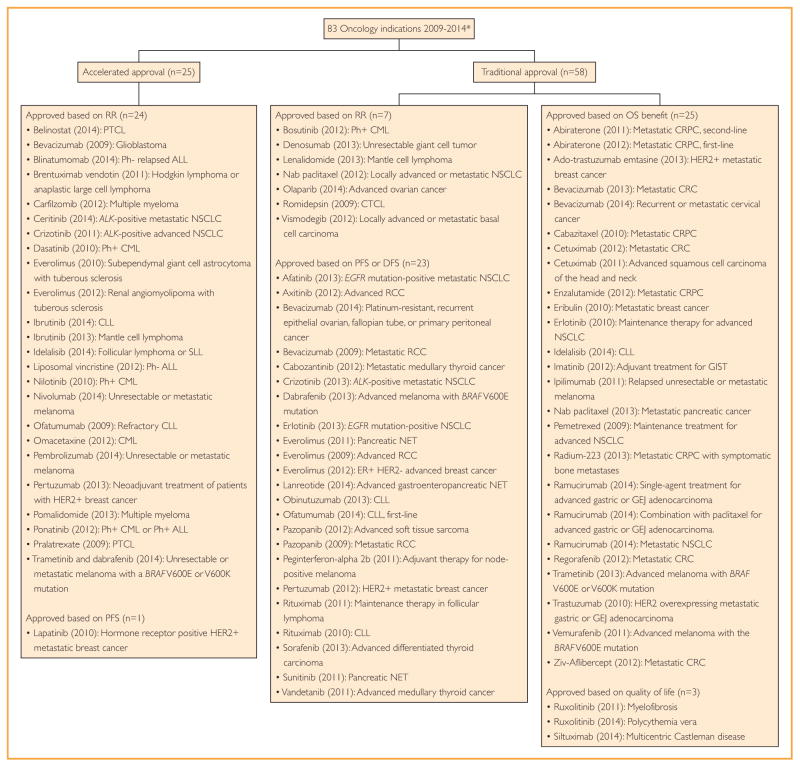
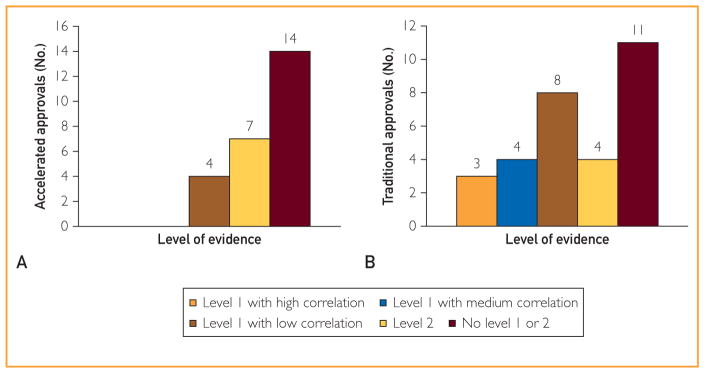
Results: Between January 1, 2009, and December 31, 2014, the FDA approved marketing applications for 55 indications based on a surrogate, of which 25 were accelerated approvals and 30 were traditional approvals. We could not find any formal analyses of the strength of the surrogate-survival correlation in 14 out of 25 accelerated approvals (56%) and 11 out of 30 traditional approvals (37%). For accelerated approvals, just 4 approvals (16%) were made where a level 1 analysis (the most robust way to validate a surrogate) had been performed, with all 4 studies reporting low correlation (r≤0.7). For traditional approvals, a level 1 analysis had been performed for 15 approvals (50%): 8 (53%) reported low correlation (r≤0.7), 4 (27%) medium correlation (r>0.7 to r<0.85), and 3 (20%) high correlation (r≥0.85) with survival.
Conclusions: The use of surrogate end points for drug approval often lacks formal empirical verification of the strength of the surrogate-survival association.
Copyright © 2016 Mayo Foundation for Medical Education and Research. All rights reserved.
Figures
References
-
- Hirschfeld S, Pazdur R. Oncology drug development: United States Food and Drug Administration perspective. Crit Rev Oncol Hematol. 2002;42(2):137–143. - PubMed
-
- Johnson JR, Williams G, Pazdur R. End points and United States Food and Drug Administration approval of oncology drugs. J Clin Oncol. 2003;21(7):1404–1411. - PubMed
-
- Pazdur R. Endpoints for assessing drug activity in clinical trials. Oncologist. 2008;13(suppl 2):19–21. - PubMed
-
- Sridhara R, Johnson JR, Justice R, Keegan P, Chakravarty A, Pazdur R. Review of oncology and hematology drug product approvals at the US Food and Drug Administration between July 2005 and December 2007. J Natl Cancer Inst. 2010;102(4):230–243. - PubMed
-
- Miller K, Wang M, Gralow J, et al. Paclitaxel plus bevacizumab versus paclitaxel alone for metastatic breast cancer. N Engl J Med. 2007;357(26):2666–2676. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
