

Impact of Completion Lymph Node Dissection on Patients with Positive Sentinel Lymph Node Biopsy in Melanoma
- PMID: 27236435
- PMCID: PMC4925269
- DOI: 10.1016/j.jamcollsurg.2016.01.045
Impact of Completion Lymph Node Dissection on Patients with Positive Sentinel Lymph Node Biopsy in Melanoma
Abstract
Background: Whether patients with positive SLNB should undergo complete lymph node dissection (CLND) is an important unanswered clinical question.
Study design: Patients diagnosed with positive SLNB at a melanoma referral center from 1991 to 2013 were studied. Outcomes of patients who underwent CLND were compared with those who did not undergo immediate CLND (observation [OBS] group).
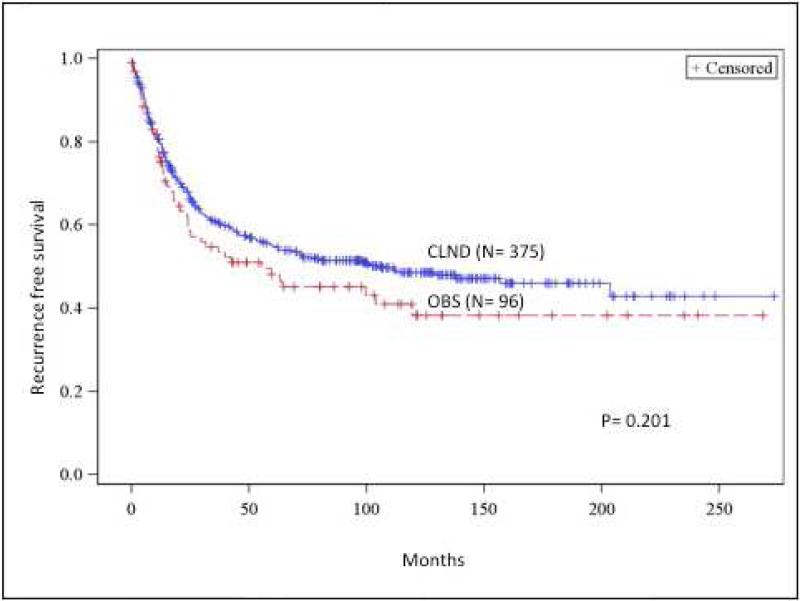
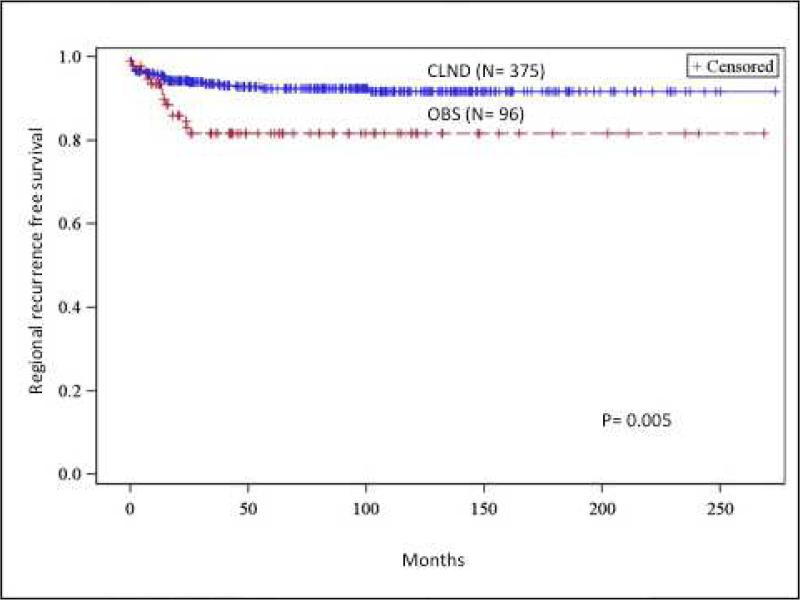
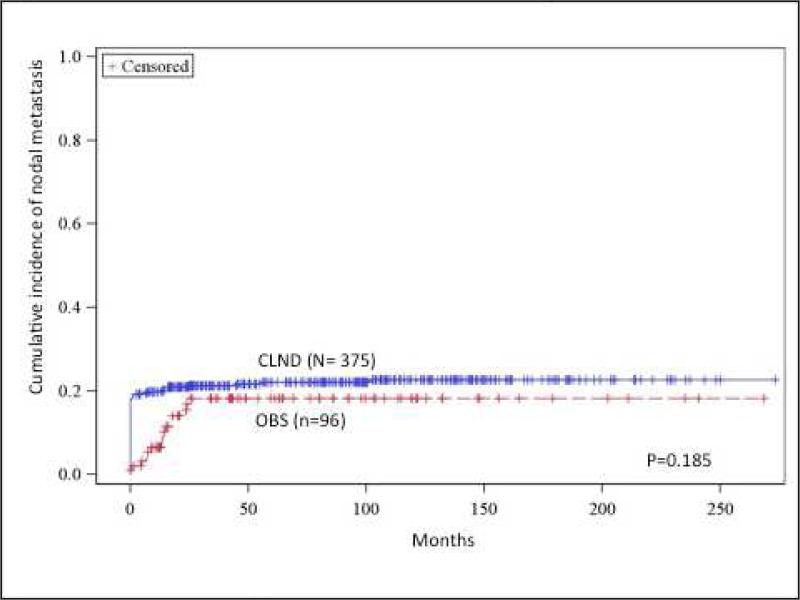
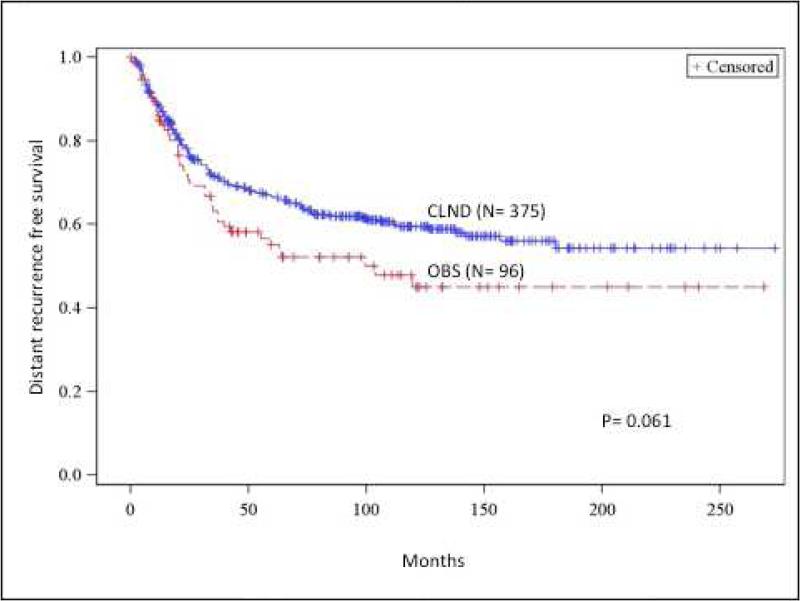
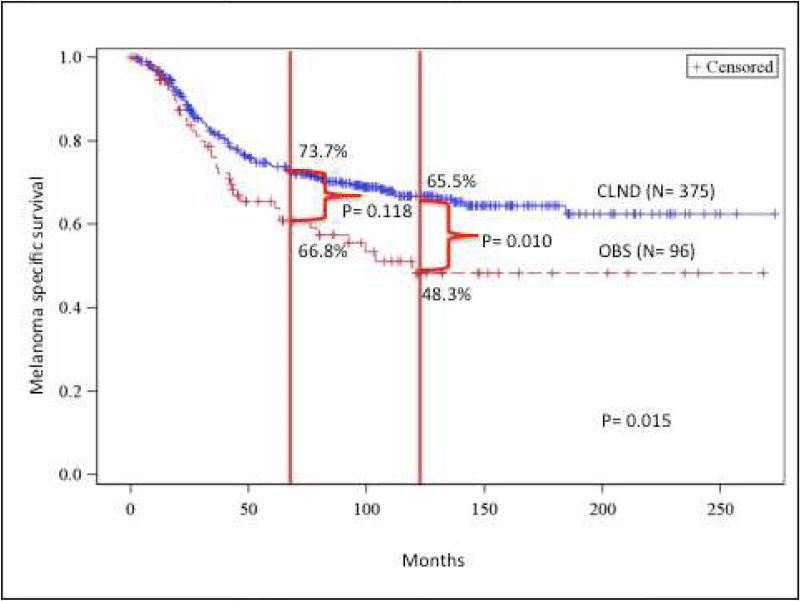
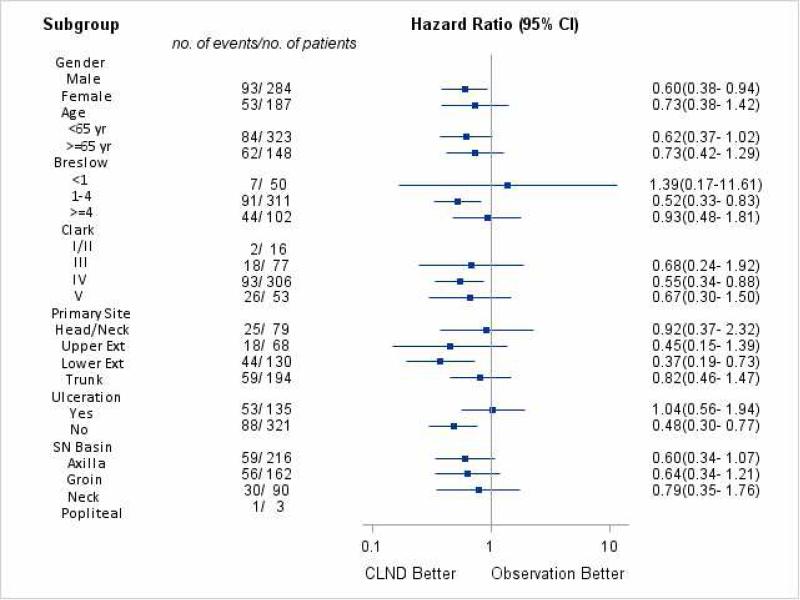
Results: There were 471 patients who had positive SLNB; 375 (79.6%) in the CLND group and 96 (20.4%) in the OBS group. The groups were similar except that the CLND group was younger and had more sentinel nodes removed. Five-year nodal recurrence-free survival was significantly better in the CLND group compared with the OBS group (93.1% vs 84.4%; p = 0.005). However, 5-year (66.4% vs 55.2%) and 10-year (59.5% vs 45.0%) distant metastasis-free survival rates were not significantly different (p = 0.061). The CLND group's melanoma-specific survival (MSS) rate was superior to that of the OBS group; 5-year MSS rates were 73.7% vs 65.5% and 10-year MSS rates were 66.8% vs 48.3% (p = 0.015). On multivariate analysis, CLND was associated with improved MSS (hazard ratio = 0.60; 95% CI, 0.40-0.89; p = 0.011) and lower nodal recurrence (hazard ratio = 0.46; 95% CI, 0.24-0.86; p = 0.016). Increased Breslow thickness, older age, ulceration, and trunk melanoma were all associated with worse outcomes. On subgroup analysis, the following factors were associated with better outcomes from CLND: male sex, nonulcerated primary, intermediate thickness, Clark level IV or lower extremity tumors.
Conclusions: Treatment of positive SLNB with CLND was associated with improved MSS and nodal recurrence rates. Follow-up beyond 5 years was needed to see a significant difference in MSS rates.
Copyright © 2016 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Discussion.J Am Coll Surg. 2016 Jul;223(1):18-9. doi: 10.1016/j.jamcollsurg.2016.04.025. J Am Coll Surg. 2016. PMID: 27345897 No abstract available.
References
-
- Morton DL CL, Wong J. Intraoperative lymphatic mapping and selective lymphadenectomy: Technical details of a new procedure for clinical stage I melanoma.. 42nd Annual Meeting of the Society of Surgical Oncology; Washington, DC. 1990 May 20-22; 1990. 1990.
-
- Nowecki ZI, Rutkowski P, Nasierowska-Guttmejer A, Ruka W. Sentinel lymph node biopsy in melanoma patients with clinically negative regional lymph nodes--one institution's experience. Melanoma Res. 2003 Feb;13(1):35–43. - PubMed
-
- Rutkowski P, Nowecki ZI, Nasierowska-Guttmejer A, Ruka W. Lymph node status and survival in cutaneous malignant melanoma--sentinel lymph node biopsy impact. Eur J Surg Oncol. 2003 Sep;29(7):611–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
