

Urine sodium concentration to predict fluid responsiveness in oliguric ICU patients: a prospective multicenter observational study
- PMID: 27236480
- PMCID: PMC4884621
- DOI: 10.1186/s13054-016-1343-0
Urine sodium concentration to predict fluid responsiveness in oliguric ICU patients: a prospective multicenter observational study
Abstract
Background: Oliguria is one of the leading triggers of fluid loading in patients in the intensive care unit (ICU). The purpose of this study was to assess the predictive value of urine Na(+) (uNa(+)) and other routine urine biomarkers for cardiac fluid responsiveness in oliguric ICU patients.
Methods: We conducted a prospective multicenter observational study in five university ICUs. Patients with urine output (UO) <0.5 ml/kg/h for 3 consecutive hours with a mean arterial pressure >65 mmHg received a fluid challenge. Cardiac fluid responsiveness was defined by an increase in stroke volume >15 % after fluid challenge. Urine and plasma biochemistry samples were examined before fluid challenge. We examined renal fluid responsiveness (defined as UO > 0.5 ml/kg/h for 3 consecutive hours) after fluid challenge as a secondary endpoint.
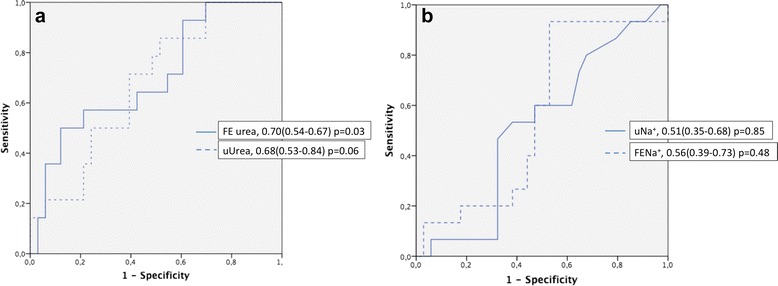
Results: Fifty-four patients (age 51 ± 37 years, Simplified Acute Physiology Score II score 40 ± 20) were included. Most patients (72 %) were not cardiac responders (CRs), and 50 % were renal responders (RRs) to fluid challenge. Patient characteristics were similar between CRs and cardiac nonresponders. uNa(+) (37 ± 38 mmol/L vs 25 ± 75 mmol/L, p = 0.44) and fractional excretion of sodium (FENa(+)) (2.27 ± 2.5 % vs 2.15 ± 5.0 %, p = 0.94) were not statistically different between those who did and those who did not respond to the fluid challenge. Areas under the receiver operating characteristic (AUROC) curves were 0.51 (95 % CI 0.35-0.68) and 0.56 (95 % CI 0.39-0.73) for uNa(+) and FENa(+), respectively. Fractional excretion of urea had an AUROC curve of 0.70 (95 % CI 0.54-0.86, p = 0.03) for CRs. Baseline UO was higher in RRs than in renal nonresponders (1.07 ± 0.78 ml/kg/3 h vs 0.65 ± 0.53 ml/kg/3 h, p = 0.01). The AUROC curve for RRs was 0.65 (95 % CI 0.53-0.78) for uNa(+).
Conclusions: In the present study, most oliguric patients were not CRs and half were not renal responders to fluid challenge. Routine urinary biomarkers were not predictive of fluid responsiveness in oliguric normotensive ICU patients.
Keywords: Acute kidney injury; Cardiac output; Fluid responsiveness; Natriuresis; Urine output.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
