

Photoplethysmography respiratory rate monitoring in patients receiving procedural sedation and analgesia for upper gastrointestinal endoscopy
- PMID: 27236561
- PMCID: PMC5500676
- DOI: 10.1007/s10877-016-9890-0
Photoplethysmography respiratory rate monitoring in patients receiving procedural sedation and analgesia for upper gastrointestinal endoscopy
Abstract
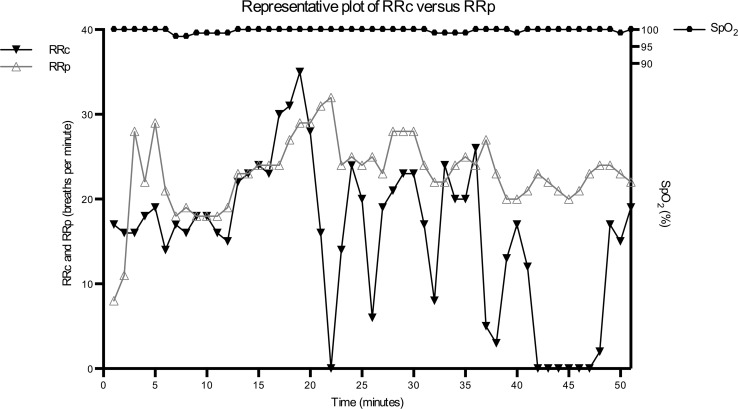
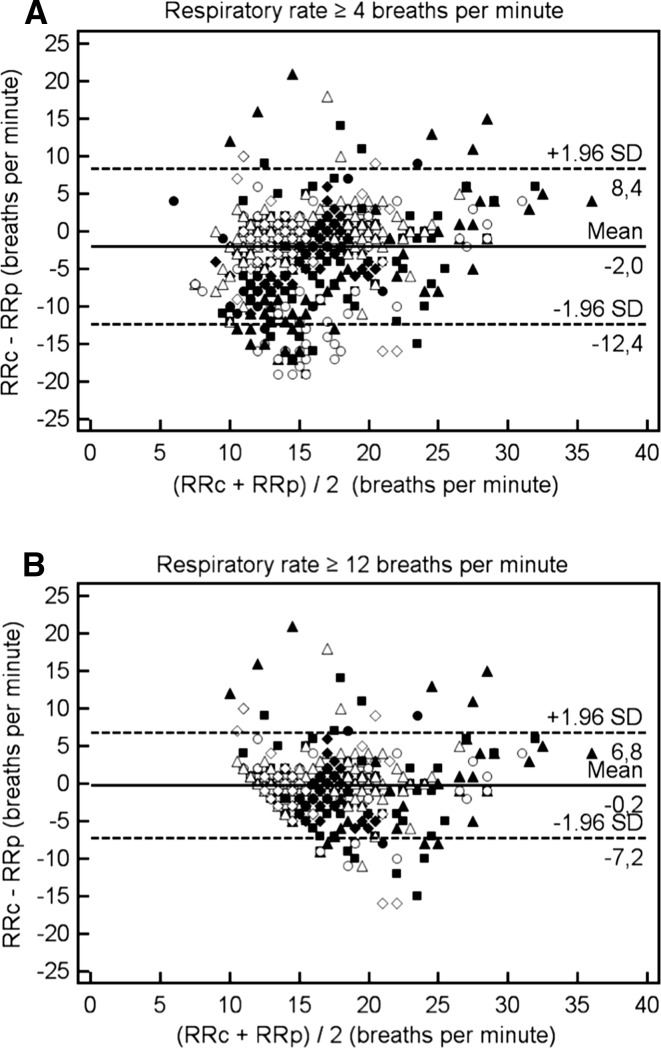
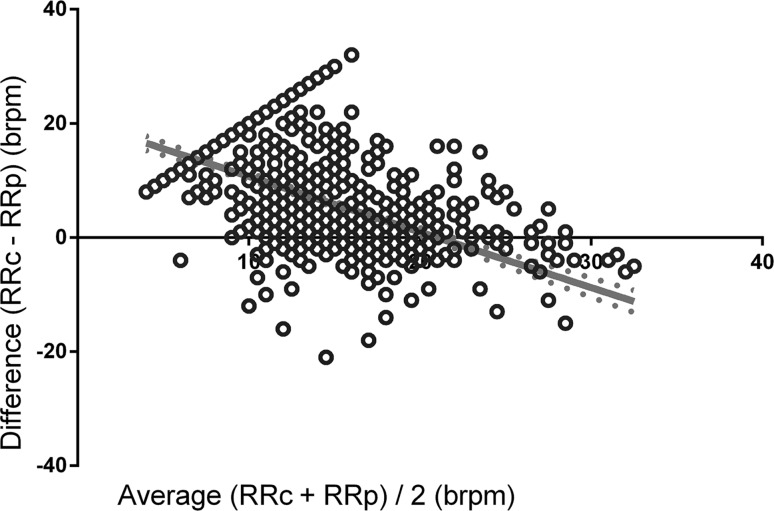
The value of capnography during procedural sedation and analgesia (PSA) for the detection of hypoxaemia during upper gastrointestinal (UGI) endoscopic procedures is limited. Photoplethysmography respiratory rate (RRp) monitoring may provide a useful alternative, but the level of agreement with capnography during PSA is unknown. We therefore investigated the level of agreement between the RRp and capnography-based RR (RRc) during PSA for UGI endoscopy. This study included patients undergoing PSA for UGI endoscopy procedures. Pulse oximetry (SpO2) and RRc were recorded in combination with Nellcor 2.0 (RRp) monitoring (Covidien, USA). Bland-Altman analysis was used to evaluate the level of agreement between RRc and RRp. Episodes of apnoea, defined as no detection of exhaled CO2 for minimal 36 s, and hypoxaemia, defined as an SpO2 < 92 %, were registered. A total of 1054 min of data from 26 patients were analysed. Bland-Altman analysis between the RRc and RRp revealed a bias of 2.25 ± 5.41 breath rate per minute (brpm), with limits of agreement from -8.35 to 12.84 brpm for an RR ≥ 4 brpm. A total of 67 apnoea events were detected. In 21 % of all apnoea events, the patient became hypoxaemic. Hypoxaemia occurred 42 times with a median length of 34 (19-141) s, and was preceded in 34 % of the cases by apnoea and in 64 % by an RRc ≥ 8 brpm. In 81 % of all apnoea events, photoplethysmography registered an RRp ≥ 4 brpm. We found a low level of agreement between capnography and the plethysmography respiratory rate during procedural sedation for UGI endoscopy. Moreover, respiratory rate derived from both the capnogram and photoplethysmogram showed a limited ability to provide warning signs for a hypoxaemic event during the sedation procedure.
Keywords: Anoxia; Apnoea; Hypoxaemia; Procedural sedation and analgesia; Respiratory rate; Sedation.
Conflict of interest statement
None of the authors have disclosures related to the present study.
Figures
References
-
- Berzin TM, Sanaka S, Barnett SR, Sundar E, Sepe PS, Jakubowski M, Pleskow DK, Chuttani R, Sawhney MS. A prospective assessment of sedation-related adverse events and patient and endoscopist satisfaction in ERCP with anesthesiologist-administered sedation. Gastrointest Endosc. 2011;73:710–717. doi: 10.1016/j.gie.2010.12.011. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
