

Severely Aggressive Children Receiving Stimulant Medication Versus Stimulant and Risperidone: 12-Month Follow-Up of the TOSCA Trial
- PMID: 27238065
- PMCID: PMC4886346
- DOI: 10.1016/j.jaac.2016.03.014
Severely Aggressive Children Receiving Stimulant Medication Versus Stimulant and Risperidone: 12-Month Follow-Up of the TOSCA Trial
Abstract
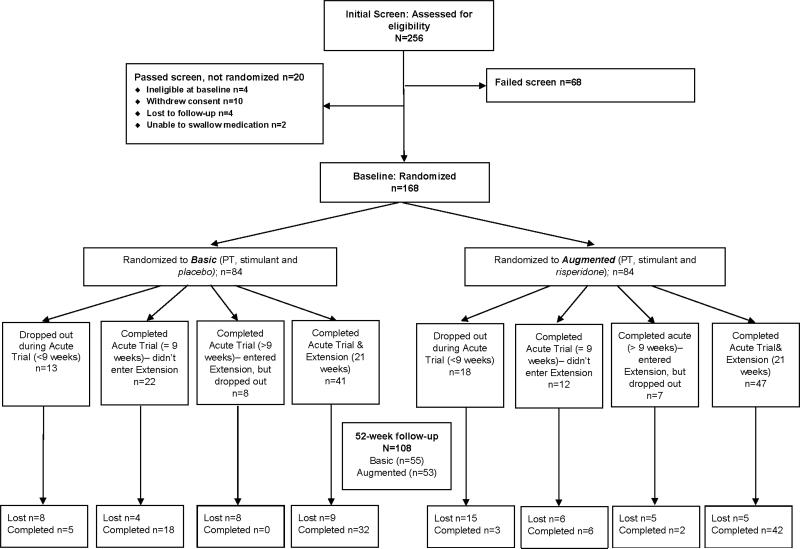
Objective: The objective of this study was to evaluate 52-week clinical outcomes of children with co-occurring attention-deficit/hyperactivity disorder (ADHD), disruptive behavior disorder, and serious physical aggression who participated in a prospective, longitudinal study that began with a controlled, 9-week clinical trial comparing the relative efficacy of parent training + stimulant medication + placebo (Basic; n = 84) versus parent training + stimulant + risperidone (Augmented; n = 84).
Method: Almost two-thirds (n = 108; 64%) of families in the 9-week study participated in week 52 follow-ups (Basic, n = 55; Augmented, n = 53) and were representative of the initial study sample. The assessment battery included caregiver and clinician ratings and laboratory tests.
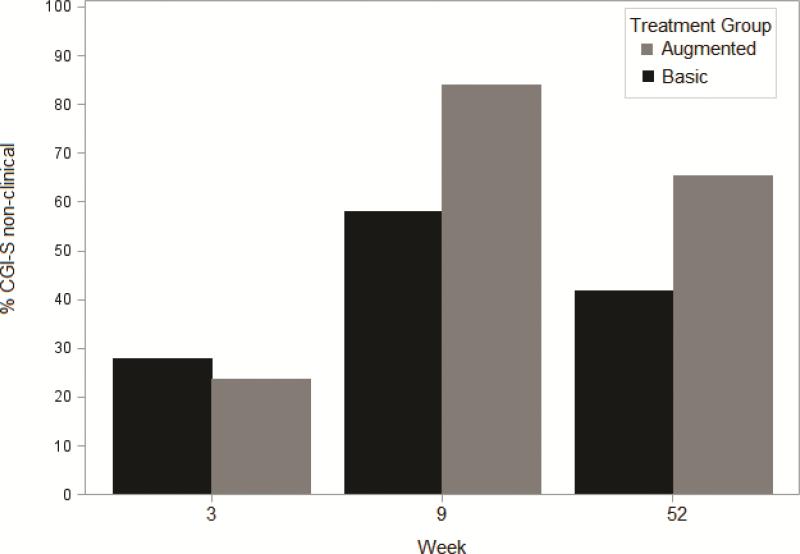
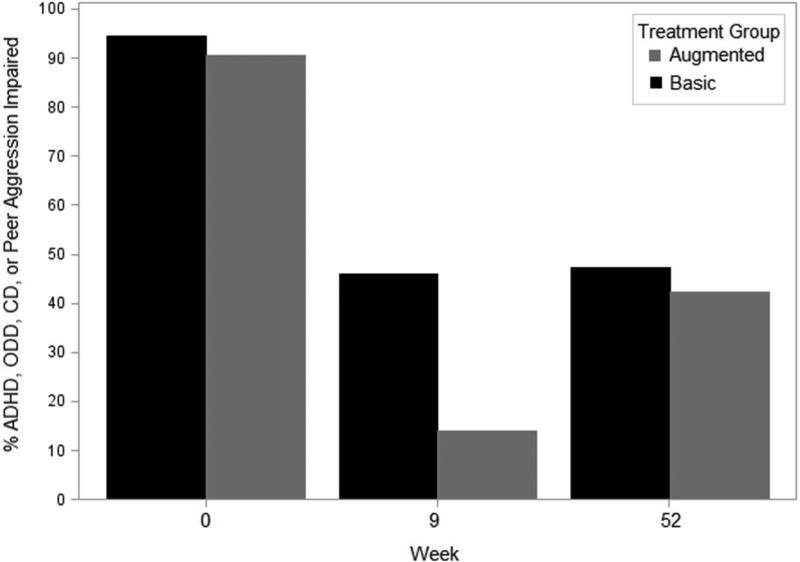
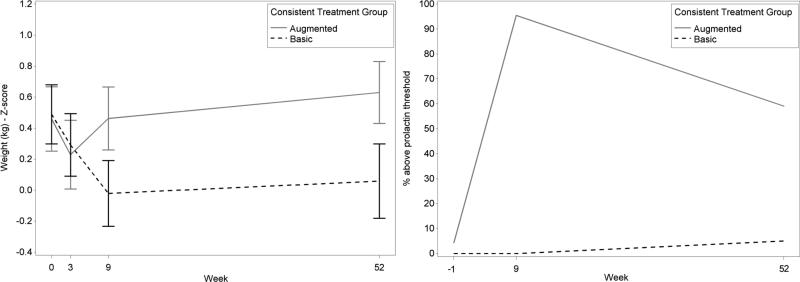
Results: Only 43% of participants in the Augmented group and 36% in the Basic group still adhered to their assigned regimen (not significant [NS]); 23% of those in the Augmented group and 11% in the Basic group were taking no medication (NS). Both randomized groups improved baseline to follow-up, but the 3 primary parent-reported behavioral outcomes showed no significant between-group differences. Exploratory analyses indicated that participants in the Augmented group (65%) were more likely (p = .02) to have a Clinical Global Impressions (CGI) severity score of 1 to 3 (i.e., normal to mildly ill) at follow-up than those in the Basic group (42%). Parents rated 45% of children as impaired often or very often from ADHD, noncompliant, or aggressive behavior. The Augmented group had elevated prolactin levels, and the Basic group had decreased weight over time. Findings were generally similar whether groups were defined by randomized assignment or follow-up treatment status.
Conclusion: Both treatment strategies were associated with clinical improvement at follow-up, and primary behavioral outcomes did not differ significantly. Many children evidenced lingering mental health concerns, suggesting the need for additional research into more effective interventions. Clinical trial registration information-Treatment of Severe Childhood Aggression (the TOSCA Study); http://clinicaltrials.gov/; NCT00796302.
Keywords: ADHD; conduct disorder; methylphenidate; oppositional defiant disorder; risperidone.
Published by Elsevier Inc.
Figures
References
-
- Bussing R, Winterstein AG. Polypharmacy in attention deficit hyperactivity disorder treatment: Current status, challenges and next steps. Curr Psychiatry Rep. 2012;14:447–449. - PubMed
-
- Duffy FF, Narrow WE, Rae DS, et al. Concomitant pharmacotherapy among youths treated in routine psychiatric practice. J Child Adolesc Psychopharmacol. 2005;15:12–25. - PubMed
-
- Connor DF, Glatt SJ, Lopez ID, Jackson D, Melloni RH., Jr Psychopharmacology and aggression. I: A meta-analysis of stimulant effects on overt/covert aggression-related behaviors in ADHD. J Am Acad Child Adolesc Psychiatry. 2002;41:253–261. - PubMed
-
- Pappadopulos E, MacIntre JC, Crismon ML, et al. Treatment Recommendations for the use of Antipsychotics for Aggressive Youth (TRAAY). Part II. J Am Acad Child Adolesc Psychiatry. 2003;42:145–161. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
