

A Diet Mimicking Fasting Promotes Regeneration and Reduces Autoimmunity and Multiple Sclerosis Symptoms
- PMID: 27239035
- PMCID: PMC4899145
- DOI: 10.1016/j.celrep.2016.05.009
A Diet Mimicking Fasting Promotes Regeneration and Reduces Autoimmunity and Multiple Sclerosis Symptoms
Abstract
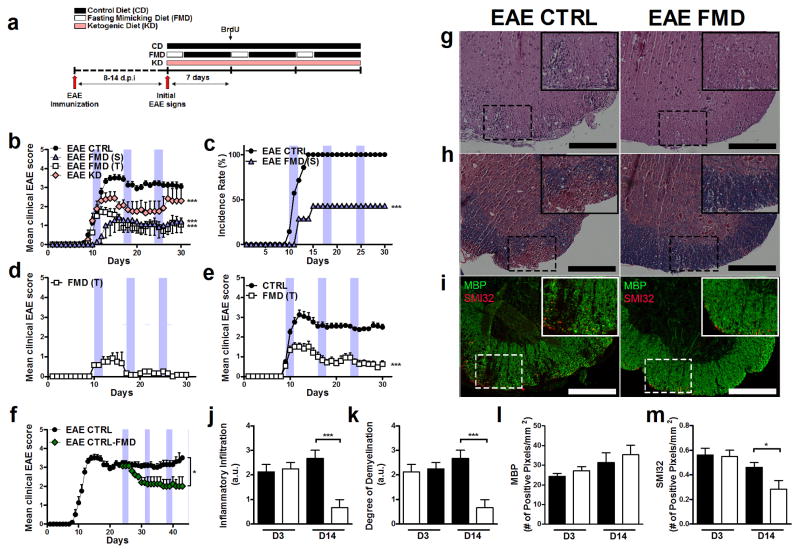
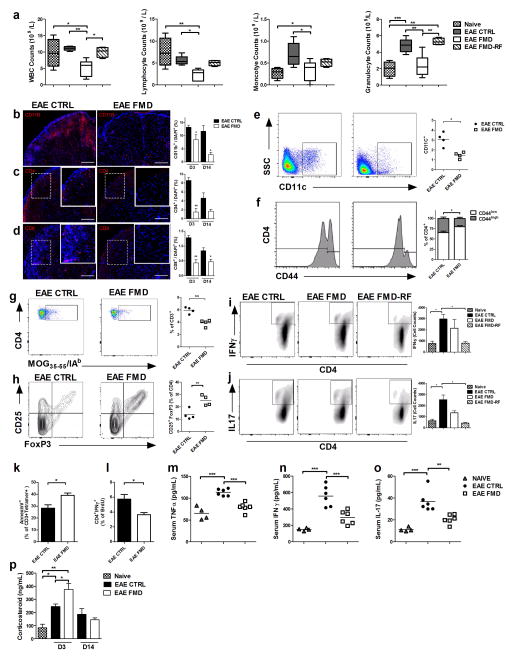
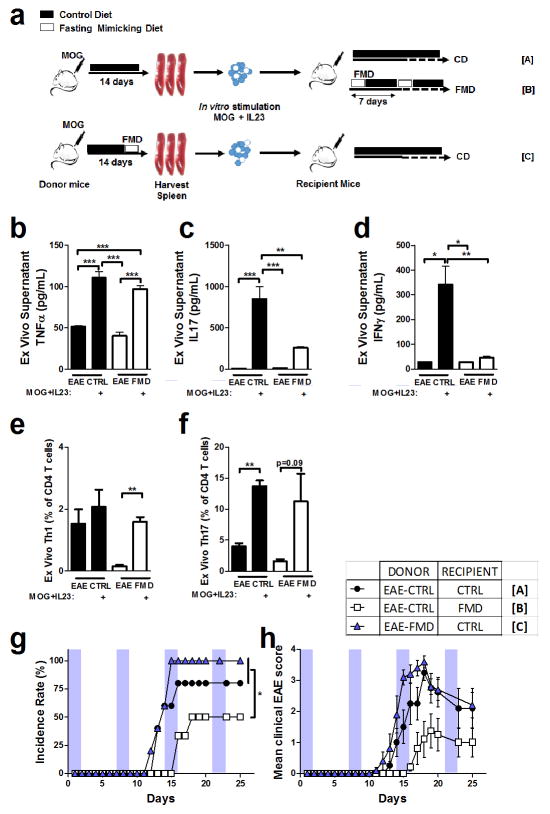
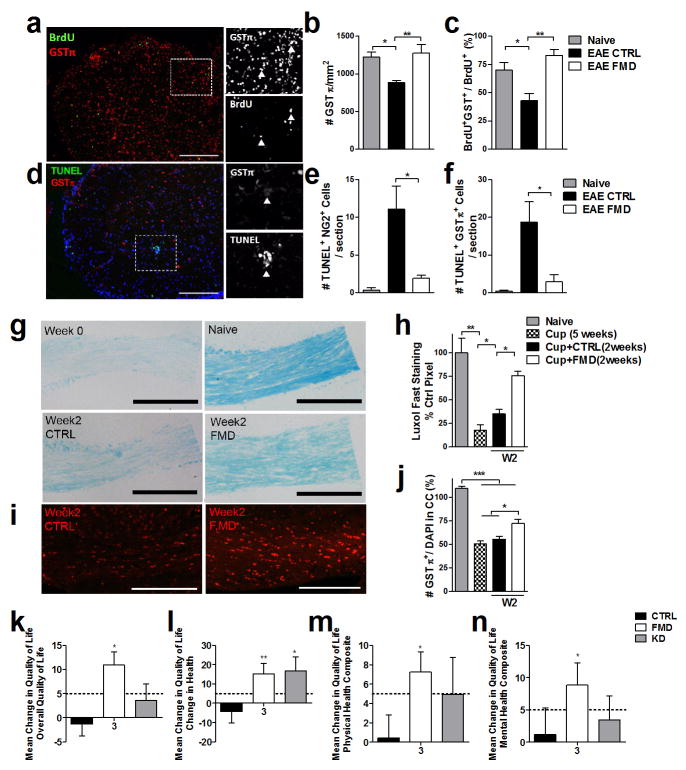
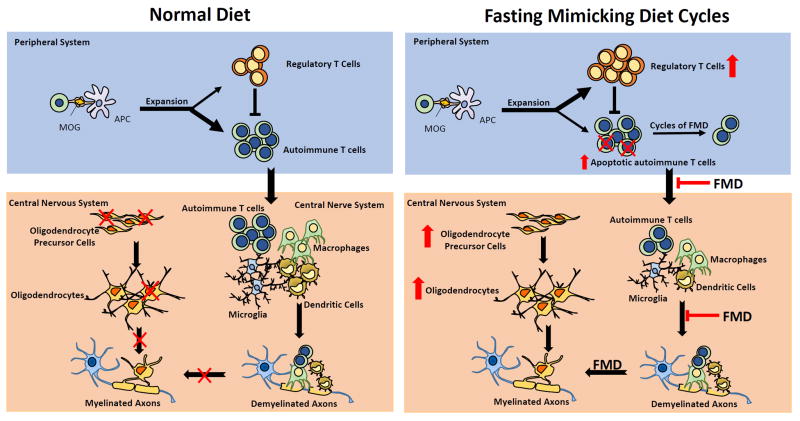
Dietary interventions have not been effective in the treatment of multiple sclerosis (MS). Here, we show that periodic 3-day cycles of a fasting mimicking diet (FMD) are effective in ameliorating demyelination and symptoms in a murine experimental autoimmune encephalomyelitis (EAE) model. The FMD reduced clinical severity in all mice and completely reversed symptoms in 20% of animals. These improvements were associated with increased corticosterone levels and regulatory T (Treg) cell numbers and reduced levels of pro-inflammatory cytokines, TH1 and TH17 cells, and antigen-presenting cells (APCs). Moreover, the FMD promoted oligodendrocyte precursor cell regeneration and remyelination in axons in both EAE and cuprizone MS models, supporting its effects on both suppression of autoimmunity and remyelination. We also report preliminary data suggesting that an FMD or a chronic ketogenic diet are safe, feasible, and potentially effective in the treatment of relapsing-remitting multiple sclerosis (RRMS) patients (NCT01538355).
Copyright © 2016 The Author(s). Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Ashwell JD, Lu FW, Vacchio MS. Glucocorticoids in T cell development and function*. Annual review of immunology. 2000;18:309–345. - PubMed
-
- Brusaferri F, Candelise L. Steroids for multiple sclerosis and optic neuritis: a meta-analysis of randomized controlled clinical trials. Journal of neurology. 2000;247:435–442. - PubMed
-
- Ce P, Gedizlioglu M, Gelal F, Coban P, Ozbek G. Avascular necrosis of the bones: an overlooked complication of pulse steroid treatment of multiple sclerosis. European journal of neurology : the official journal of the European Federation of Neurological Societies. 2006;13:857–861. - PubMed
-
- Chang A, Tourtellotte WW, Rudick R, Trapp BD. Premyelinating oligodendrocytes in chronic lesions of multiple sclerosis. The New England journal of medicine. 2002;346:165–173. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
