

Neurocritical care update
- PMID: 27239312
- PMCID: PMC4884370
- DOI: 10.1186/s40560-016-0141-8
Neurocritical care update
Erratum in
-
Erratum to: Neurocritical care update.J Intensive Care. 2016 Jul 25;4:49. doi: 10.1186/s40560-016-0168-x. eCollection 2016. J Intensive Care. 2016. PMID: 27462399 Free PMC article.
Abstract
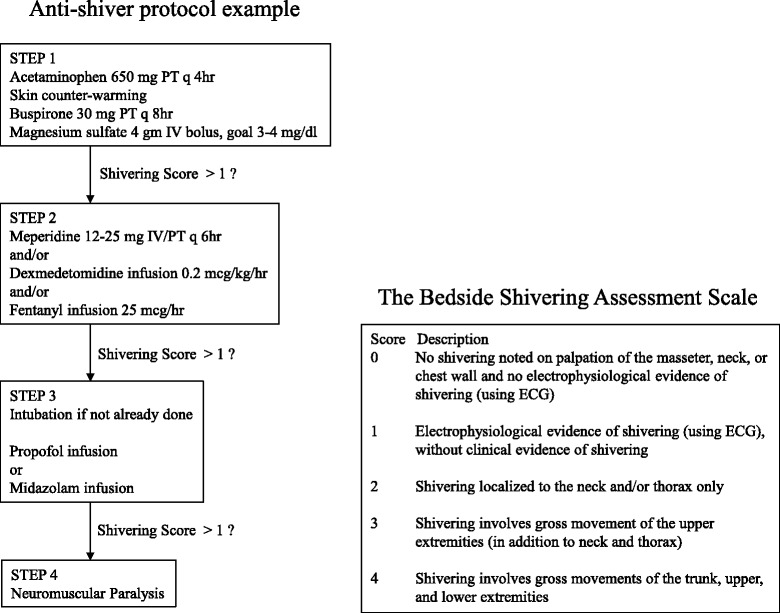
This update comprises six important topics under neurocritical care that require reevaluation. For post-cardiac arrest brain injury, the evaluation of the injury and its corresponding therapy, including temperature modulation, is required. Analgosedation for target temperature management is an essential strategy to prevent shivering and minimizes endogenous stress induced by catecholamine surges. For severe traumatic brain injury, the diverse effects of therapeutic hypothermia depend on the complicated pathophysiology of the condition. Continuous electroencephalogram monitoring is an essential tool for detecting nonconvulsive status epilepticus in the intensive care unit (ICU). Neurocritical care, including advanced hemodynamic monitoring, is a fundamental approach for delayed cerebral ischemia following subarachnoid hemorrhage. We must be mindful of the high percentage of ICU patients who may develop sepsis-associated brain dysfunction.
Keywords: Electroencephalogram monitoring; Neurocritical care; Nonconvulsive status epilepticus; Review; Sepsis-associated brain dysfunction; Shivering; Target temperature management.
Figures
References
-
- Wada T, Gando S, Mizugaki A, Yanagida Y, Jesmin S, Yokota H, Ieko M. Coagulofibrinolytic changes in patients with disseminated intravascular coagulation associated with post-cardiac arrest syndrome—fibrinolytic shutdown and insufficient activation of fibrinolysis lead to organ dysfunction. Thromb Res. 2013;132(1):e64–9. doi: 10.1016/j.thromres.2013.05.010. - DOI - PubMed
-
- Nunnally M, Jaeschke R, Bellingan G, Lacroix J, Mourvillier B, Rodriguez-Vega G, Rubertsson S, Vassilakopoulos T, Weinert C, Zanotti-Cavazzoni S, et al. Targeted temperature management in critical care: a report and recommendations from five professional societies. Crit Care Med. 2011;39(5):1113–25. doi: 10.1097/CCM.0b013e318206bab2. - DOI - PubMed
-
- Peberdy MA, Callaway CW, Neumar RW, Geocadin RG, Zimmerman JL, Donnino M, Gabrielli A, Silvers SM, Zaritsky AL, Merchant R, et al. Part 9: post-cardiac arrest care: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(18 Suppl 3):S768–86. doi: 10.1161/CIRCULATIONAHA.110.971002. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
