

Automatic speech analysis for the assessment of patients with predementia and Alzheimer's disease
- PMID: 27239498
- PMCID: PMC4876915
- DOI: 10.1016/j.dadm.2014.11.012
Automatic speech analysis for the assessment of patients with predementia and Alzheimer's disease
Abstract
Background: To evaluate the interest of using automatic speech analyses for the assessment of mild cognitive impairment (MCI) and early-stage Alzheimer's disease (AD).
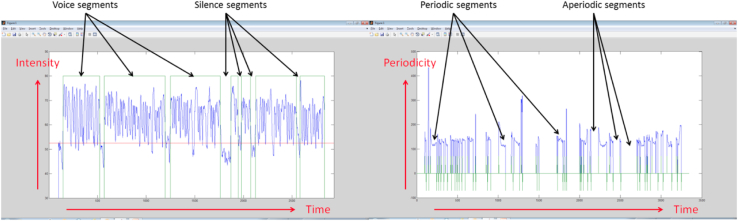
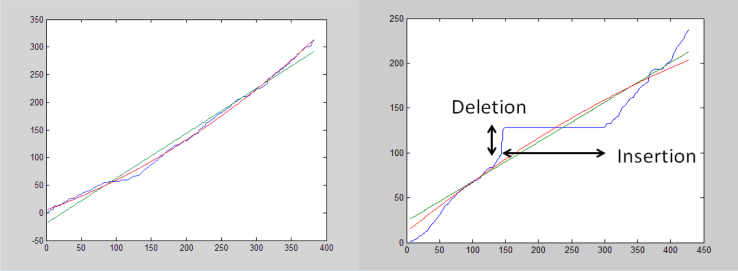
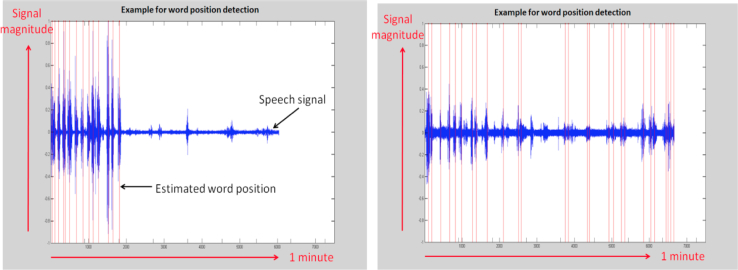
Methods: Healthy elderly control (HC) subjects and patients with MCI or AD were recorded while performing several short cognitive vocal tasks. The voice recordings were processed, and the first vocal markers were extracted using speech signal processing techniques. Second, the vocal markers were tested to assess their "power" to distinguish among HC, MCI, and AD. The second step included training automatic classifiers for detecting MCI and AD, using machine learning methods and testing the detection accuracy.
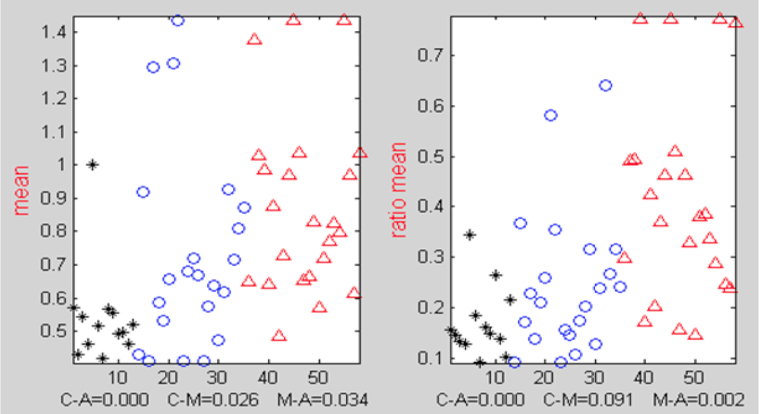
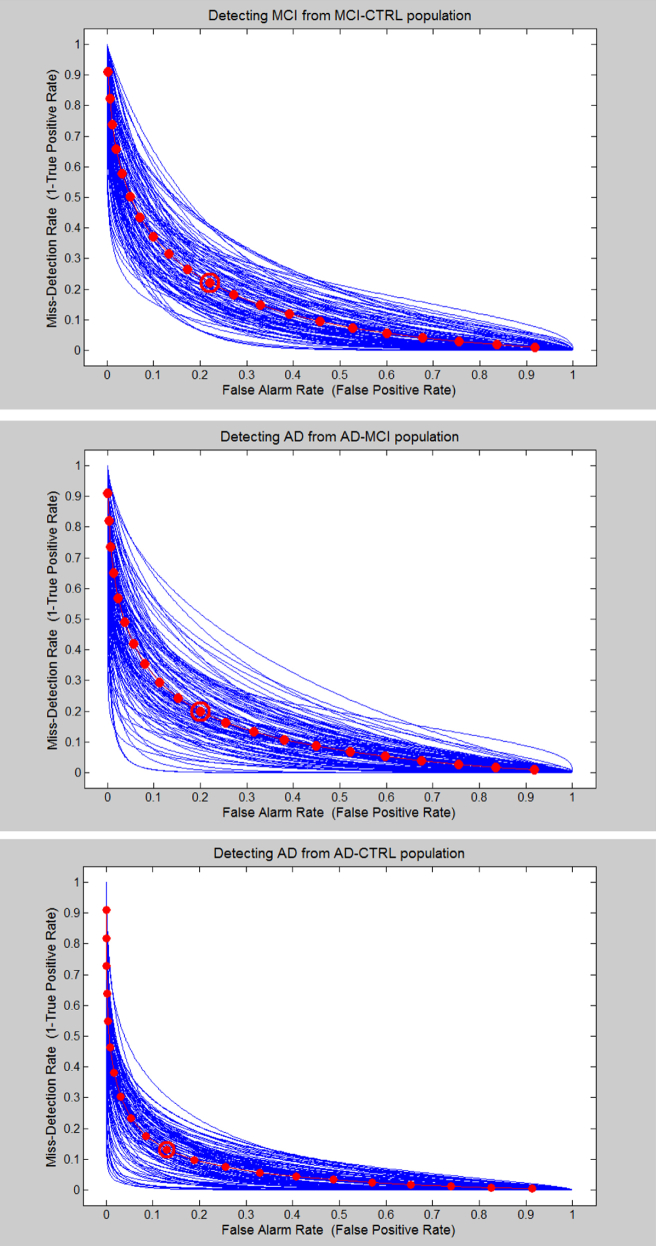
Results: The classification accuracy of automatic audio analyses were as follows: between HCs and those with MCI, 79% ± 5%; between HCs and those with AD, 87% ± 3%; and between those with MCI and those with AD, 80% ± 5%, demonstrating its assessment utility.
Conclusion: Automatic speech analyses could be an additional objective assessment tool for elderly with cognitive decline.
Keywords: Alzheimer's; Assessment; Audio; Dementia; Information and communication technology (ICT); Mild cognitive impairment; Speech analyses; Vocal task.
Figures
References
-
- Braaten A.J., Parsons T.D., McCue R., Sellers A., Burns W.J. Neurocognitive differential diagnosis of dementing diseases: Alzheimer's dementia, vascular dementia, frontotemporal dementia, and major depressive disorder. Int J Neurosci. 2006;116:1271–1293. - PubMed
-
- Forbes K.E., Venneri A., Shanks M.F. Distinct patterns of spontaneous speech deterioration: An early predictor of Alzheimer's disease. Brain Cogn. 2002;48:356–361. - PubMed
-
- Yakhia M., Konig A., van der Flier W.M., Friedman L., Robert P.H., David R. Actigraphic motor activity in mild cognitive impairment patients carrying out short functional activity tasks: Comparison between mild cognitive impairment with and without depressive symptoms. J Alzheimers Dis. 2014;40:869–875. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources