

The Anticipated Clinical and Economic Effects of 90-90-90 in South Africa
- PMID: 27240120
- PMCID: PMC5012932
- DOI: 10.7326/M16-0799
The Anticipated Clinical and Economic Effects of 90-90-90 in South Africa
Abstract
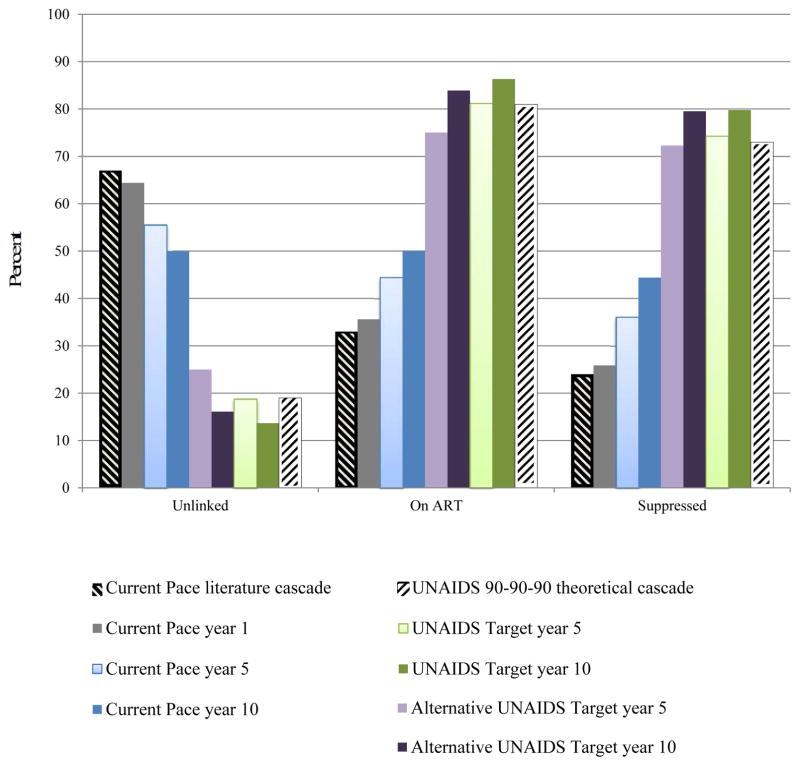
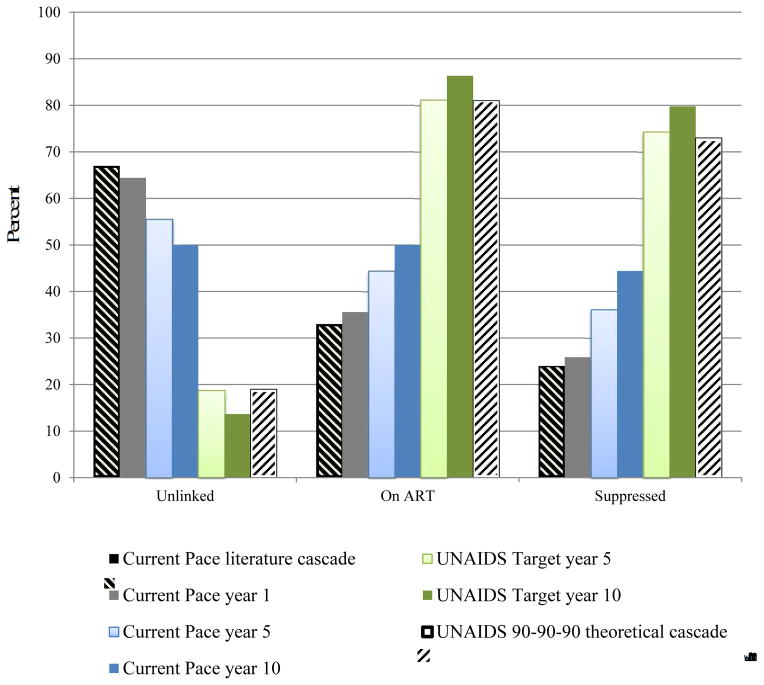
Background: The Joint United Nations Programme on HIV/AIDS (UNAIDS) 90-90-90 global treatment target aims to achieve 73% virologic suppression among HIV-infected persons worldwide by 2020.
Objective: To estimate the clinical and economic value of reaching this ambitious goal in South Africa, by using a microsimulation model of HIV detection, disease, and treatment.
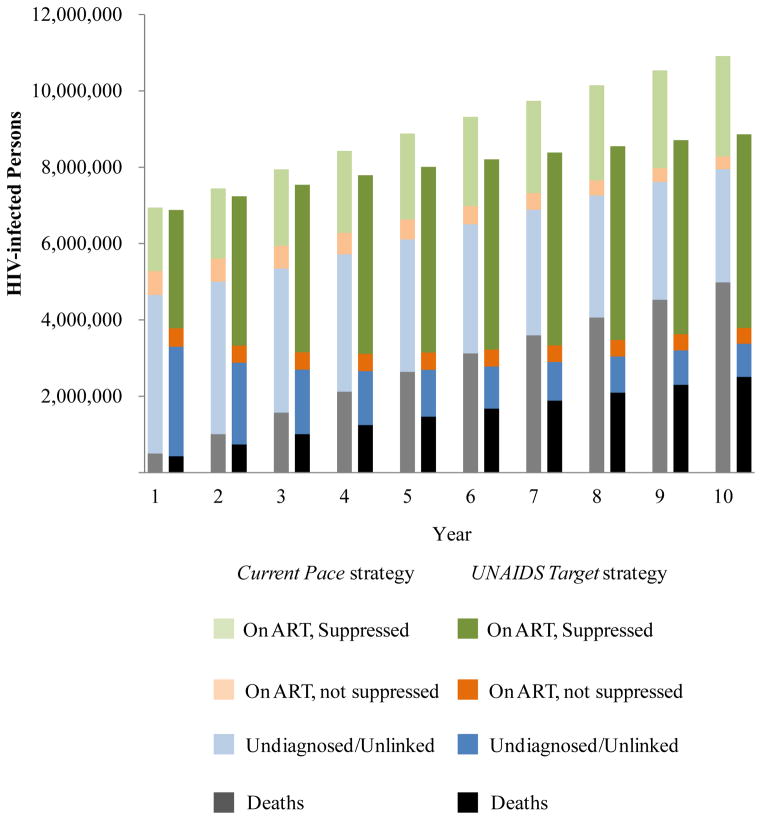
Design: Modeling of the "current pace" strategy, which simulates existing scale-up efforts and gradual increases in overall virologic suppression from 24% to 36% in 5 years, and the UNAIDS target strategy, which simulates 73% virologic suppression in 5 years.
Data sources: Published estimates and South African survey data on HIV transmission rates (0.16 to 9.03 per 100 person-years), HIV-specific age-stratified fertility rates (1.0 to 9.1 per 100 person-years), and costs of care ($11 to $31 per month for antiretroviral therapy and $20 to $157 per month for routine care).
Target population: South African HIV-infected population, including incident infections over the next 10 years.
Perspective: Modified societal perspective, excluding time and productivity costs.
Time horizon: 5 and 10 years.
Intervention: Aggressive HIV case detection, efficient linkage to care, rapid treatment scale-up, and adherence and retention interventions toward the UNAIDS target strategy.
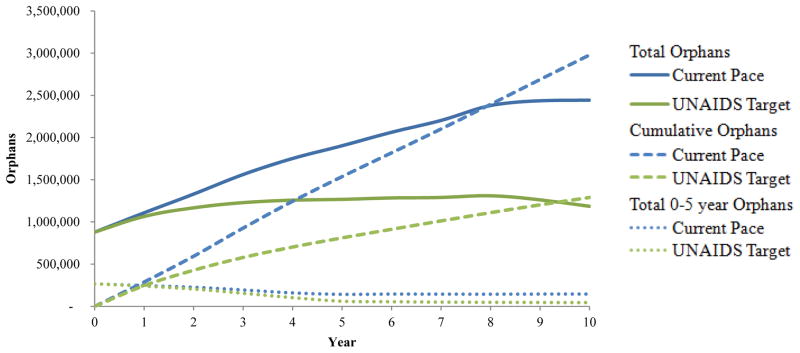
Outcome measures: HIV transmissions, deaths, years of life saved, maternal orphans, costs (2014 U.S. dollars), and cost-effectiveness.
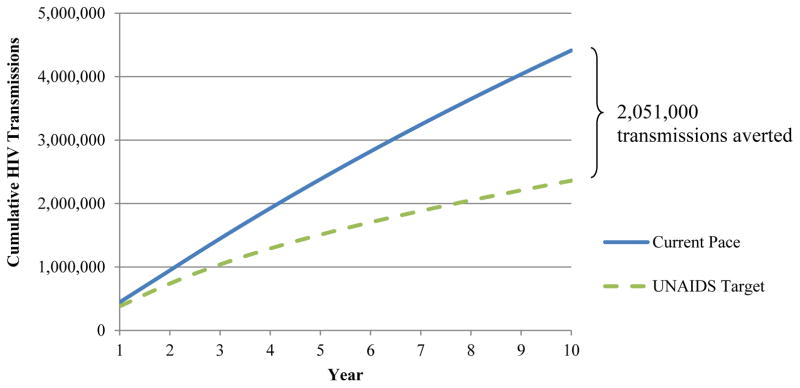
Results of base-case analysis: Compared with the current pace strategy, over 5 years the UNAIDS target strategy would avert 873 000 HIV transmissions, 1 174 000 deaths, and 726 000 maternal orphans while saving 3 002 000 life-years; over 10 years, it would avert 2 051 000 HIV transmissions, 2 478 000 deaths, and 1 689 000 maternal orphans while saving 13 340 000 life-years. The additional budget required for the UNAIDS target strategy would be $7.965 billion over 5 years and $15.979 billion over 10 years, yielding an incremental cost-effectiveness ratio of $2720 and $1260 per year of life saved, respectively.
Results of sensitivity analysis: Outcomes generally varied less than 20% from base-case outcomes when key input parameters were varied within plausible ranges.
Limitation: Several pathways may lead to 73% overall virologic suppression; these were examined in sensitivity analyses.
Conclusion: Reaching the 90-90-90 HIV suppression target would be costly but very effective and cost-effective in South Africa. Global health policymakers should mobilize the political and economic support to realize this target.
Primary funding source: National Institutes of Health and the Steve and Deborah Gorlin MGH Research Scholars Award.
Figures
References
-
- 90-90-90: an ambitious treatment target to help end the AIDS epidemic. Geneva, Switzerland: Joint United Nations Programme on HIV/AIDS (UNAIDS); 2014. [Accessed March 30, 2016]. at http://www.unaids.org/sites/default/files/media_asset/90-90-90_en_0.pdf.
-
- Piot P, Abdool Karim SS, Hecht R, Legido-Quigley H, Buse K, Stover J, et al. Defeating AIDS—advancing global health. Lancet. 2015;386(9989):171–218. - PubMed
-
- Long L, Fox M, Sanne I, Rosen S. The high cost of second-line antiretroviral therapy for HIV/AIDS in South Africa. AIDS. 2010;24(6):915–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials