

Predictors of Major Morbidity or Mortality After Resection for Esophageal Cancer: A Society of Thoracic Surgeons General Thoracic Surgery Database Risk Adjustment Model
- PMID: 27240449
- PMCID: PMC5016796
- DOI: 10.1016/j.athoracsur.2016.04.055
Predictors of Major Morbidity or Mortality After Resection for Esophageal Cancer: A Society of Thoracic Surgeons General Thoracic Surgery Database Risk Adjustment Model
Abstract
Background: The purpose of this analysis was to revise the model for perioperative risk for esophagectomy for cancer utilizing The Society of Thoracic Surgeons General Thoracic Surgery Database to provide enhanced risk stratification and quality improvement measures for contributing centers.
Methods: The Society of Thoracic Surgeons General Thoracic Surgery Database was queried for all patients treated for esophageal cancer with esophagectomy between July 1, 2011, and June 30, 2014. Multivariable risk models for major morbidity, perioperative mortality, and combined morbidity and mortality were created with the inclusion of surgical approach as a risk factor.
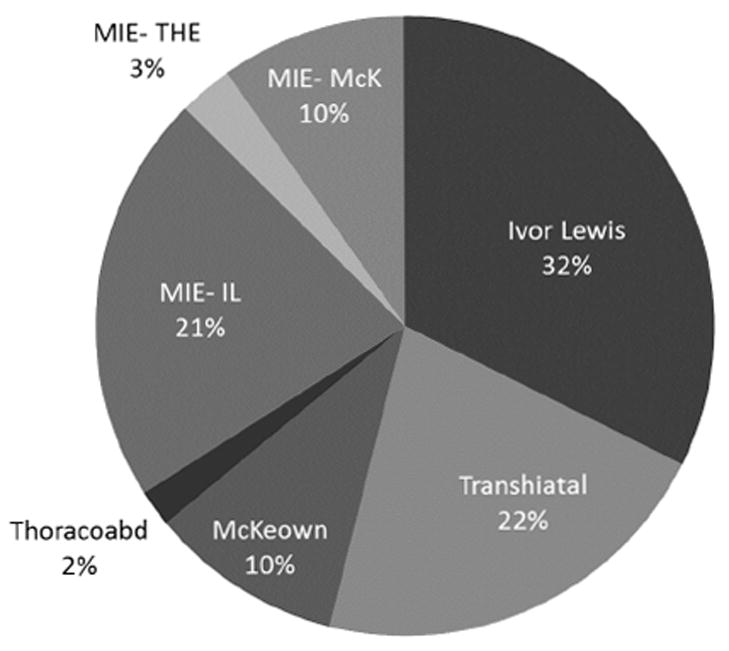
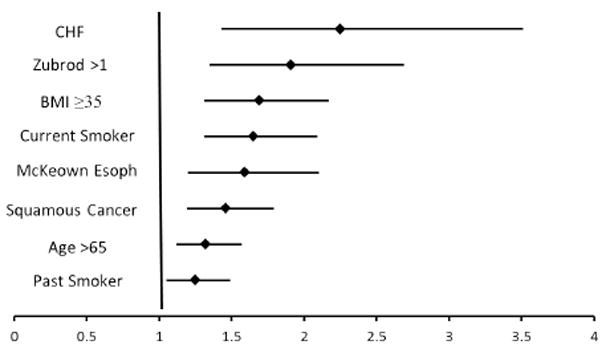
Results: In all, 4,321 esophagectomies were performed by 164 participating centers. The most common procedures included Ivor Lewis (32.5%), transhiatal (21.7%), minimally invasive esophagectomy, Ivor Lewis type (21.4%), and McKeown (10.0%). Sixty-nine percent of patients received induction therapy. Perioperative mortality (inpatient and 30-day) was 135 of 4,321 (3.4%). Major morbidity occurred in 1,429 patients (33.1%). Major morbidities include unexpected return to operating (15.6%), anastomotic leak (12.9%), reintubation (12.2%), initial ventilation beyond 48 hours (3.5%), pneumonia (12.2%), renal failure (2.0%), and recurrent laryngeal nerve paresis (2.0%). Statistically significant predictors of combined major morbidity or mortality included age more than 65 years, body mass index 35 kg/m(2) or greater, preoperative congestive heart failure, Zubrod score greater than 1, McKeown esophagectomy, current or former smoker, and squamous cell histology.
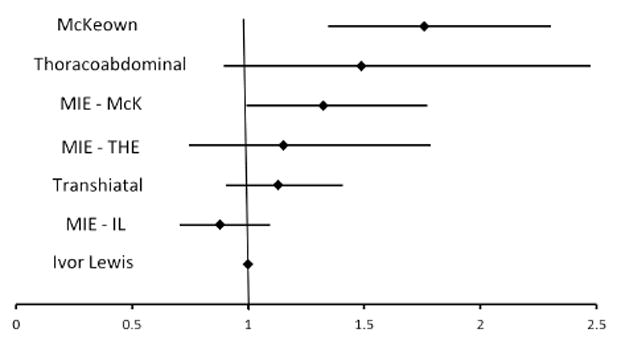
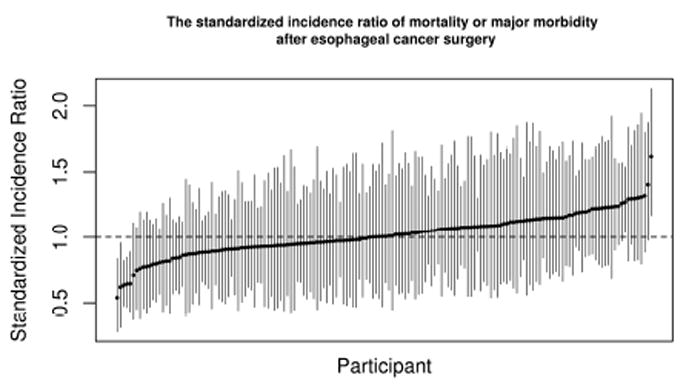
Conclusion: Thoracic surgeons participating in The Society of Thoracic Surgeons General Thoracic Surgery Database perform esophagectomy with low morbidity and mortality. McKeown esophagectomy is an independent predictor of combined postoperative morbidity or mortality. Revised predictors for perioperative outcome were identified to facilitate quality improvement processes and hospital comparisons.
Copyright © 2016 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- SEER Stat Fact Sheets: Esophageal Cancer. 2015
-
- Pennathur A, et al. Oesophageal carcinoma. Lancet. 2013;381(9864):400–12. - PubMed
-
- Low DE, et al. International Consensus on Standardization of Data Collection for Complications Associated With Esophagectomy: Esophagectomy Complications Consensus Group (ECCG) Ann Surg. 2015;262(2):286–94. - PubMed
-
- Wright CD, et al. Predictors of major morbidity and mortality after esophagectomy for esophageal cancer: a Society of Thoracic Surgeons General Thoracic Surgery Database risk adjustment model. J Thorac Cardiovasc Surg. 2009;137(3):587–95. discussion 596. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
