

Raltegravir in second-line antiretroviral therapy in resource-limited settings (SELECT): a randomised, phase 3, non-inferiority study
- PMID: 27240787
- PMCID: PMC4914044
- DOI: 10.1016/S2352-3018(16)30011-X
Raltegravir in second-line antiretroviral therapy in resource-limited settings (SELECT): a randomised, phase 3, non-inferiority study
Abstract
Background: For second-line antiretroviral therapy, WHO recommends a boosted protease inhibitor plus nucleoside or nucleotide reverse transcriptase inhibitors (NRTIs). However, concerns about toxicity and cross-resistance motivated a search for regimens that do not contain NRTIs. We aimed to assess whether boosted lopinavir plus raltegravir would be non-inferior to boosted lopinavir plus NRTIs for virological suppression in resource-limited settings.
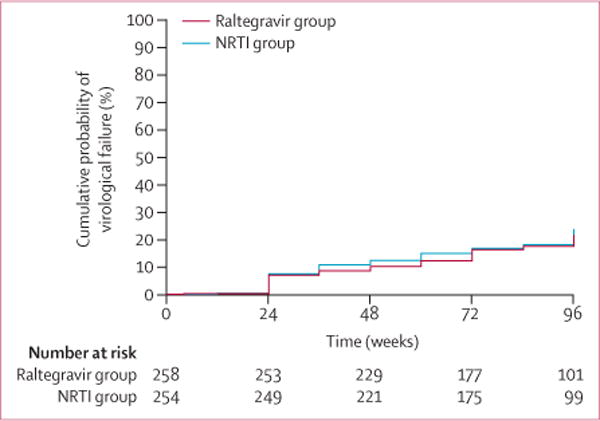
Methods: A5273 was a randomised, open-label, phase 3, non-inferiority study at 15 AIDS Clinical Trials Group (ACTG) research sites in nine resource-limited countries (three sites each in India and South Africa, two each in Malawi and Peru, and one each in Brazil, Kenya, Tanzania, Thailand, and Zimbabwe). Adults with plasma HIV-1 RNA concentrations of at least 1000 copies per mL after at least 24 weeks on a regimen based on a non-NRTI inhibitor were randomly assigned (1:1) to receive oral ritonavir-boosted lopinavir (100 mg ritonavir, 400 mg lopinavir) plus 400 mg raltegravir twice a day (raltegravir group) or to ritonavir-boosted lopinavir plus two or three NRTIs selected from an algorithm (eg, zidovudine after failure with tenofovir and vice versa; NRTI group). Randomised group assignment was done with a computer algorithm concealed to site personnel, and stratified by HIV-1 RNA viral load, CD4 cell count, and intention to use zidovudine, with the groups balanced by each site. The primary endpoint was time to confirmed virological failure (two measurements of HIV-1 RNA viral load >400 copies per mL) at or after week 24 in the intention-to-treat population. Non-inferiority (10% margin) was assessed by comparing the cumulative probability of virological failure by 48 weeks. This trial was registered with ClinicalTrials.gov, NCT01352715.
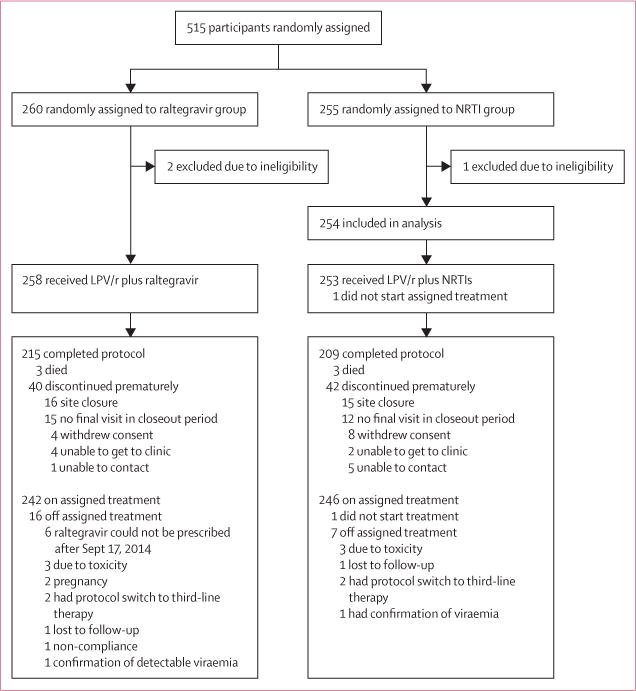
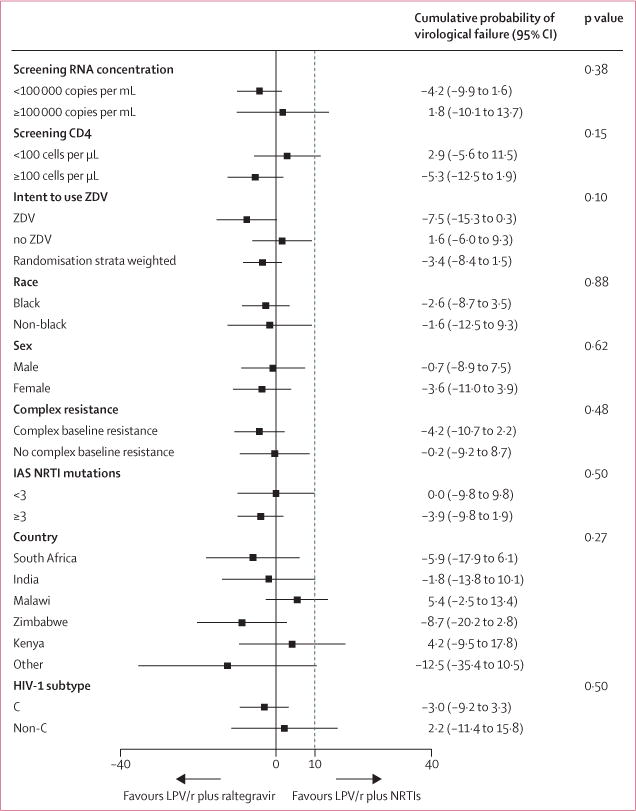
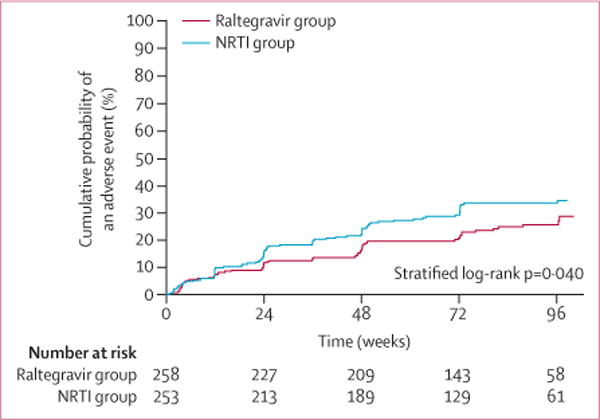
Findings: Between March 13, 2012, and Oct 2, 2013, we randomly assigned 515 participants: 260 to the raltegravir group and 255 to the NRTI group; two participants in the raltegravir group and one in the NRTI group were excluded from analyses because of ineligibility. By the end of follow-up (October, 2014), 96 participants had virological failure (46 in the raltegravir group and 50 in the NRTI group). By 48 weeks, the cumulative probability of virological failure was 10·3% (95% CI 6·5-14·0) in the raltegravir group and 12·4% (8·3-16·5) in the NRTI group, with a weighted difference of -3·4% (-8·4 to 1·5), indicating that raltegravir was non-inferior, but not superior, to NRTIs. 62 (24%) participants in the raltegravir group and 81 (32%) in the NRTI group had grade 3 or higher adverse events; 19 (7%) and 29 (11%), respectively, had serious adverse events. Three participants in each group died, all from HIV-related causes.
Interpretation: In settings with extensive NRTI resistance but no available resistance testing, our data support WHO's recommendation for ritonavir-boosted lopinavir plus NRTI for second-line antiretroviral therapy. Ritonavir-boosted lopinavir plus raltegravir is an appropriate alternative, especially if NRTI use is limited by toxicity.
Funding: National Institutes of Health.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Conflict of interest statement
AMLR has received salary support from Johnson & Johnson (Peru) and Merck Sharp & Dohme (Peru). BT has received research grants and honoraria from ViiV, and honoraria from Gilead Sciences, GlaxoSmithKline, and Janssen. CLW has received honoraria from Abbvie/Abbott, Celera, and Merck Sharp & Dohme. JWM has received funds from Gilead Sciences, support from Cocrystal Pharma, and has a patent for 3’Azido Purine Nucleotide Prodrugs for treatment of viral infections (number 8, 815, 829). ACC has received research support from Bristol-Myers Squibb, Merck Sharp & Dohme, and Roche Molecular Systems; and honoraria from Merck Sharp & Dohme for data and safety monitoring board membership. All other authors declare no competing interests.
Figures
Comment in
-
Raltegravir in second-line ART in resource-limited settings.Lancet HIV. 2016 Jun;3(6):e240-1. doi: 10.1016/S2352-3018(16)30014-5. Epub 2016 Apr 18. Lancet HIV. 2016. PMID: 27240783 No abstract available.
References
-
- UNAIDS. “15 by 15” A Global Target Achieved. http://www.unaids.org/sites/default/files/media_asset/UNAIDS_15by15_en.pdf (accessed Sept 8, 2015).
-
- World Health Organization. Guideline on when to start antiretroviral therapy and on pre-exposure prophylaxis for HIV. 2015 Sep; http://www.who.int/hiv/pub/guidelines/earlyrelease-arv/en/ (accessed Oct 13, 2015). - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U01 AI069423/AI/NIAID NIH HHS/United States
- U01 AI069438/AI/NIAID NIH HHS/United States
- UM1 AI069476/AI/NIAID NIH HHS/United States
- UM1 AI068634/AI/NIAID NIH HHS/United States
- UM1 AI069481/AI/NIAID NIH HHS/United States
- UM1 AI069453/AI/NIAID NIH HHS/United States
- UM1 AI069463/AI/NIAID NIH HHS/United States
- UM1 AI106701/AI/NIAID NIH HHS/United States
- UM1 AI108568/AI/NIAID NIH HHS/United States
- UM1 AI069417/AI/NIAID NIH HHS/United States
- UM1 AI069497/AI/NIAID NIH HHS/United States
- UM1 AI069436/AI/NIAID NIH HHS/United States
- UM1 AI068636/AI/NIAID NIH HHS/United States
- U01 AI069497/AI/NIAID NIH HHS/United States
- UM1 AI069423/AI/NIAID NIH HHS/United States
- U01 AI069463/AI/NIAID NIH HHS/United States
- UM1 AI069432/AI/NIAID NIH HHS/United States
- U01 AI069481/AI/NIAID NIH HHS/United States
- UM1 AI069438/AI/NIAID NIH HHS/United States
- U01 AI069484/AI/NIAID NIH HHS/United States
- UM1 AI069471/AI/NIAID NIH HHS/United States
- UM1 AI069518/AI/NIAID NIH HHS/United States
- U01 AI069432/AI/NIAID NIH HHS/United States
- UM1 AI069399/AI/NIAID NIH HHS/United States
- U01 AI068636/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
