

Ablating atrial fibrillation: A translational science perspective for clinicians
- PMID: 27241354
- PMCID: PMC4996702
- DOI: 10.1016/j.hrthm.2016.05.026
Ablating atrial fibrillation: A translational science perspective for clinicians
Abstract
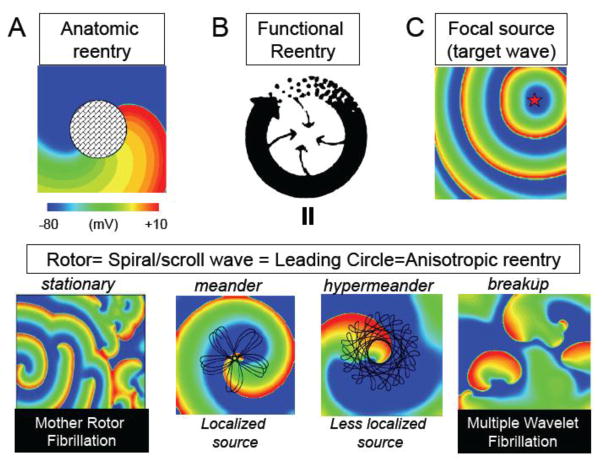
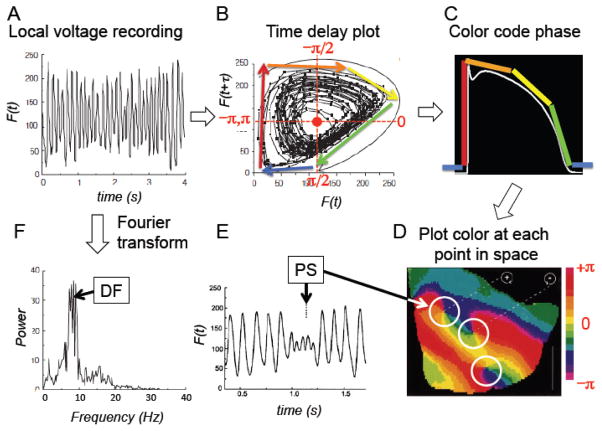
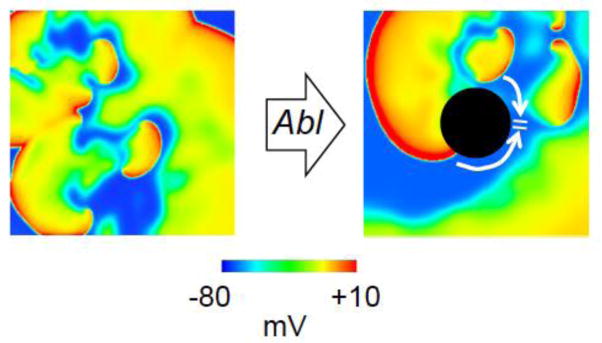
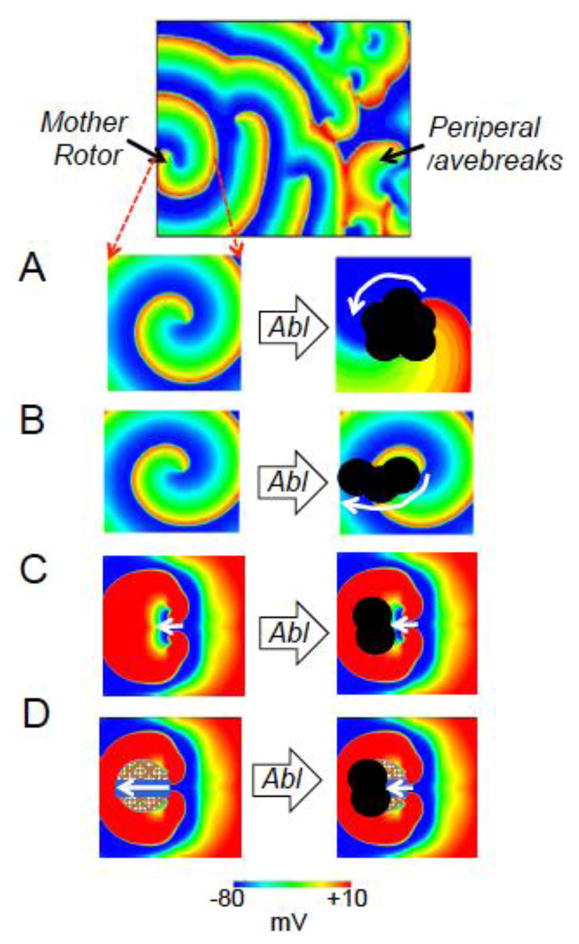
Although considerable progress has been made in developing ablation approaches to cure atrial fibrillation (AF), outcomes are still suboptimal, especially for persistent and long-lasting persistent AF. In this topical review, we review the arrhythmia mechanisms, both reentrant and nonreentrant, that are potentially relevant to human AF at various stages/settings. We describe arrhythmia mapping techniques used to distinguish between the different mechanisms, with a particular focus on the detection of rotors. We discuss which arrhythmia mechanisms are likely to respond to ablation, and the challenges and prospects for improving upon current ablation strategies to achieve better outcomes.
Keywords: Ablation; Arrhythmia; Atrial fibrillation; Automaticity; Fibrosis; Reentry; Rotor; Triggered activity.
Copyright © 2016 Heart Rhythm Society. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
None
Figures
References
-
- Haissaguerre M, Jais P, Shah DC, Takahashi A, Hocini M, Quiniou G, Garrigue S, Le Mouroux A, Le Metayer P, Clementy J. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998;339:659–666. - PubMed
-
- Verma A, Jiang CY, Betts TR, et al. Approaches to catheter ablation for persistent atrial fibrillation. N Engl J Med. 2015;372:1812–1822. - PubMed
-
- Narayan SM, Krummen DE, Shivkumar K, Clopton P, Rappel WJ, Miller JM. Treatment of atrial fibrillation by the ablation of localized sources: CONFIRM (Conventional Ablation for Atrial Fibrillation With or Without Focal Impulse and Rotor Modulation) trial. J Am Coll Cardiol. 2012;60:628–636. - PMC - PubMed
-
- Narayan SM, Baykaner T, Clopton P, Schricker A, Lalani GG, Krummen DE, Shivkumar K, Miller JM. Ablation of rotor and focal sources reduces late recurrence of atrial fibrillation compared with trigger ablation alone: extended follow-up of the CONFIRM trial (Conventional Ablation for Atrial Fibrillation With or Without Focal Impulse and Rotor Modulation) Journal of the American College of Cardiology. 2014;63:1761–1768. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
