

Acceptability, Feasibility, and Cost of Telemedicine for Nonacute Headaches: A Randomized Study Comparing Video and Traditional Consultations
- PMID: 27241876
- PMCID: PMC4906238
- DOI: 10.2196/jmir.5221
Acceptability, Feasibility, and Cost of Telemedicine for Nonacute Headaches: A Randomized Study Comparing Video and Traditional Consultations
Abstract
Background: The feasibility of telemedicine in diagnosing and treating nonacute headaches, such as primary headaches (migraine and tension-type) and medication-overuse headaches has not been previously investigated. By eliminating the need of travel to specialists, telemedicine may offer significant time and money savings.
Objectives: Our objective was to estimate the acceptance of telemedicine and investigate the feasibility and cost savings of telemedicine consultations in diagnosing and treating nonacute headaches.
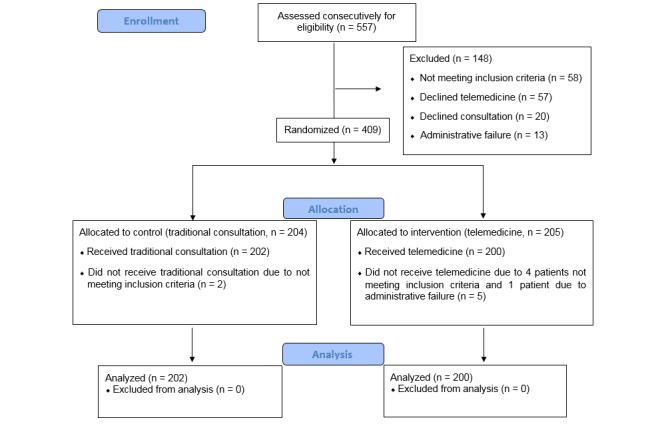
Methods: From September 2012 to March 2015, nonacute headache patients from Northern Norway who were referred to neurologists through an electronic application system were consecutively screened and randomized to participate in either telemedicine or traditional specialist visits. All patients were consulted by two neurologists at the neurological department in Tromsø University Hospital. Feasibility outcomes were compared between telemedicine and traditional groups. Baseline characteristics and costs were then compared between rural and urban patients. Travel costs were calculated by using the probabilistic method of the Norwegian traveling agency: the cheapest means of public transport for each study participant. Loss of pay was calculated based on the Norwegian full-time employee's average salary: < 3.5 hours=a half day's salary, > 3.5 hours spent on travel and consultation=one day's salary. Distance and time spent on travel were estimated by using Google Maps.
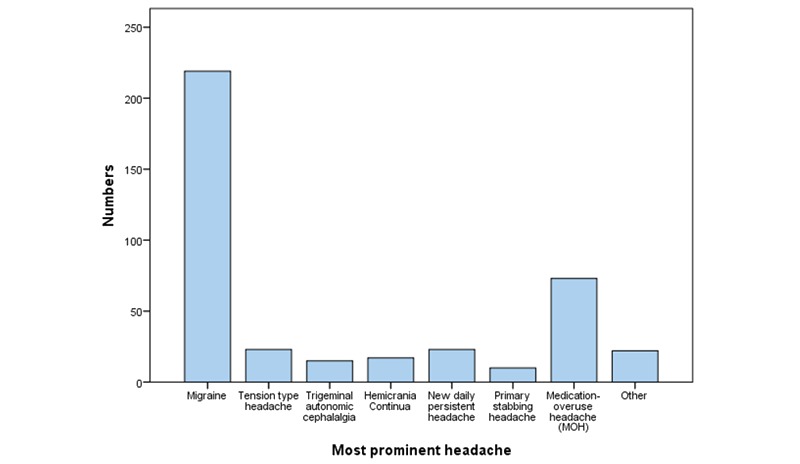
Results: Of 557 headache patients screened, 479 were found eligible and 402 accepted telemedicine participation (83.9%, 402/479) and were included in the final analyses. Of these, 202 received traditional specialist consultations and 200 received telemedicine. All patients in the telemedicine group were satisfied with the video quality, and 198 (99%, 198/200) were satisfied with the sound quality. The baseline characteristics as well as headache diagnostics and follow-up appointments, and the investigation, advice, and prescription practices were not statistically different between the two randomized groups. In addition, telemedicine consultations were shorter than traditional visits (38.8 vs 43.7 min, P<.001). The travel cost per rural individual (292/402, 73%) was €249, and estimated lost income was €234 per visit. The travel cost in the urban area (110/402, 27%) was €6, and estimated lost income was €117 per visit. The median traveling distance for rural patients was 526 km (range 1892 km), and the median traveling time was 7.8 hours (range 27.3 hours). Rural patients had a longer waiting time than urban patients (64 vs 47 days, P=.001), and fewer women were referred from rural areas (P=.04). Rural women reported higher pain scores than urban women (P=.005).
Conclusion: Our study shows that telemedicine is an accepted, feasible, time-saving, and cost-saving alternative to traditional specialist consultations for nonacute headaches.
Trial registration: Clinicaltrials.gov NCT02270177; http://clinicaltrials.gov/ct2/show/NCT02270177 (Archived by WebCite at http://www.webcitation.org/6hmoHGo9Q).
Keywords: burden; consultation; cost; feasibility; headache; management; randomization; rural; telemedicine.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Rasmussen BK, Jensen R, Schroll M, Olesen J. Epidemiology of headache in a general population--a prevalence study. J Clin Epidemiol. 1991;44(11):1147–57.0895-4356(91)90147-2 - PubMed
-
- Global Burden of Disease Study 2013 Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015 Aug 22;386(9995):743–800. doi: 10.1016/S0140-6736(15)60692-4. http://europepmc.org/abstract/MED/26063472 S0140-6736(15)60692-4 - DOI - PMC - PubMed
-
- Institute for Health Metrics and Evaluation (IHME) [2016-01-22]. http://ghdx.healthdata.org/global-burden-disease-study-2013-gbd-2013-dat... .
-
- Bekkelund SI, Albretsen C. Evaluation of referrals from general practice to a neurological department. Fam Pract. 2002 Jun;19(3):297–9. http://fampra.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=11978723 - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
