

Combined IL-21-primed polyclonal CTL plus CTLA4 blockade controls refractory metastatic melanoma in a patient
- PMID: 27242164
- PMCID: PMC4925025
- DOI: 10.1084/jem.20152021
Combined IL-21-primed polyclonal CTL plus CTLA4 blockade controls refractory metastatic melanoma in a patient
Abstract
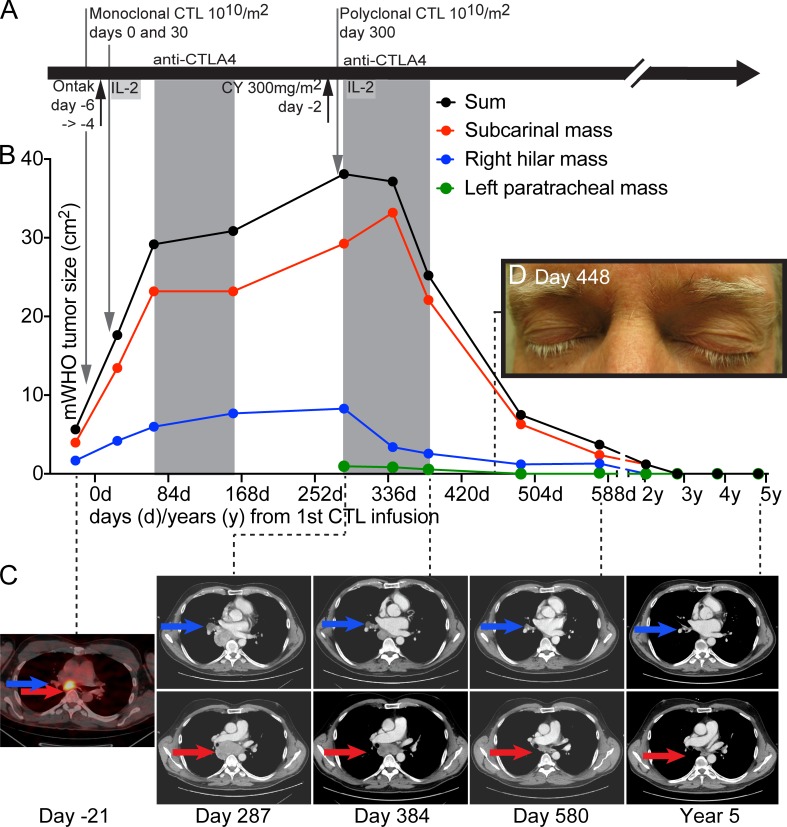
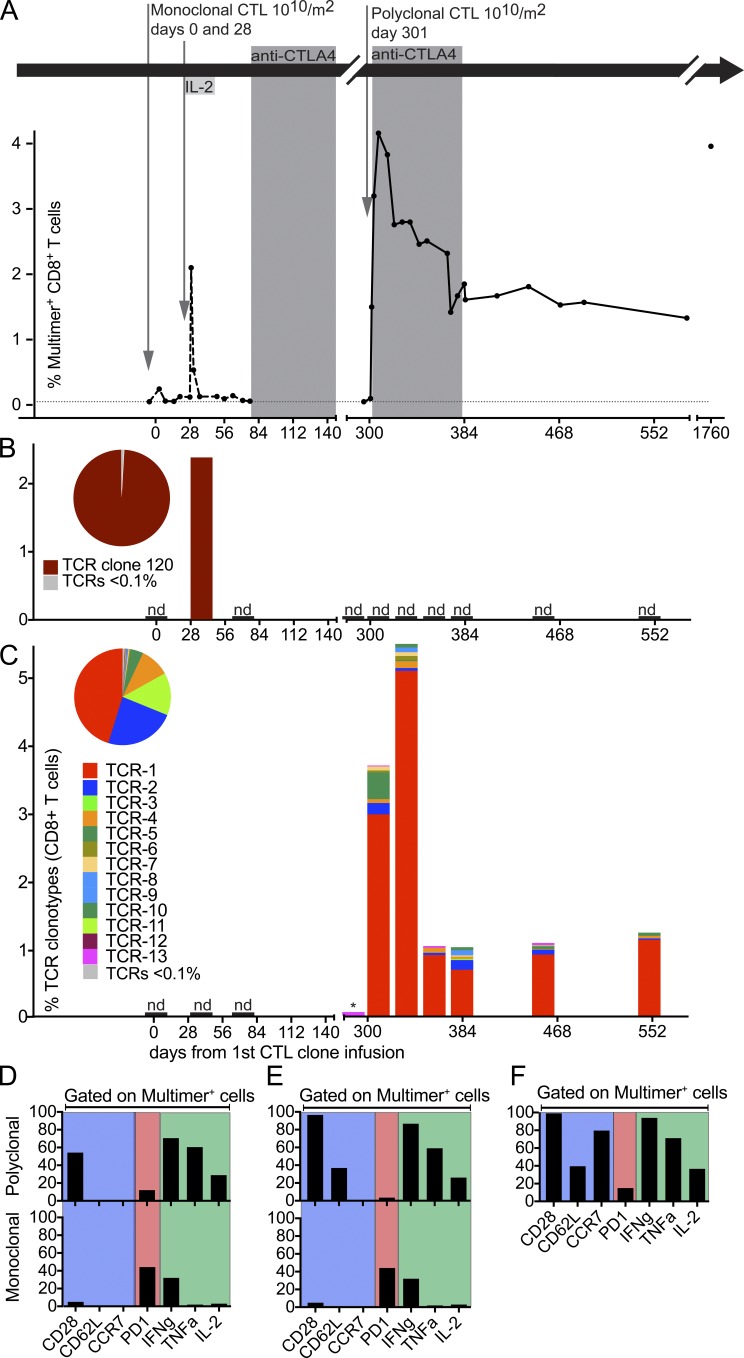
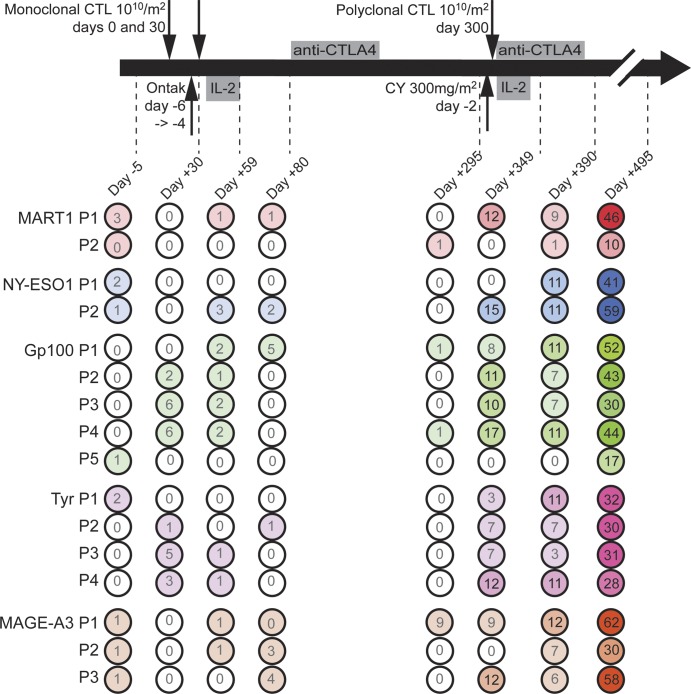
Adoptive transfer of peripheral blood-derived, melanoma-reactive CD8(+) cytotoxic T lymphocytes (CTLs) alone is generally insufficient to eliminate bulky tumors. Similarly, monotherapy with anti-CTLA4 infrequently yields sustained remissions in patients with metastatic melanoma. We postulated that a bolus of enhanced IL-21-primed polyclonal antigen-specific CTL combined with CTLA4 blockade might boost antitumor efficacy. In this first-in-human case study, the combination successfully led to a durable complete remission (CR) in a patient whose disease was refractory to both monoclonal CTL and anti-CTLA4. Long-term persistence and sustained anti-tumor activity of transferred CTL, as well as responses to nontargeted antigens, confirmed mutually beneficial effects of the combined treatment. In this first-in-human study, Chapuis et al. demonstrate that the combination of adoptive cellular therapy with CTLA4 blockade induces long-term remission in a melanoma patient resistant to both modalities administered serially and individually.
© 2016 Chapuis et al.
Figures
Comment in
-
Combination immunotherapy for cancer.J Exp Med. 2016 Jun 27;213(7):1115. doi: 10.1084/jem.2137insight2. J Exp Med. 2016. PMID: 27353088 Free PMC article. No abstract available.
References
-
- Chapuis A.G., Thompson J.A., Margolin K.A., Rodmyre R., Lai I.P., Dowdy K., Farrar E.A., Bhatia S., Sabath D.E., Cao J., et al. 2012. Transferred melanoma-specific CD8+ T cells persist, mediate tumor regression, and acquire central memory phenotype. Proc. Natl. Acad. Sci. USA. 109:4592–4597. 10.1073/pnas.1113748109 - DOI - PMC - PubMed
-
- Chapuis A.G., Ragnarsson G.B., Nguyen H.N., Chaney C.N., Pufnock J.S., Schmitt T.M., Duerkopp N., Roberts I.M., Pogosov G.L., Ho W.Y., et al. 2013. Transferred WT1-reactive CD8+ T cells can mediate antileukemic activity and persist in post-transplant patients. Sci. Transl. Med. 5:174ra27 10.1126/scitranslmed.3004916 - DOI - PMC - PubMed
-
- Freeman G.J., Long A.J., Iwai Y., Bourque K., Chernova T., Nishimura H., Fitz L.J., Malenkovich N., Okazaki T., Byrne M.C., et al. 2000. Engagement of the PD-1 immunoinhibitory receptor by a novel B7 family member leads to negative regulation of lymphocyte activation. J. Exp. Med. 192:1027–1034. 10.1084/jem.192.7.1027 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
