

A QI Initiative to Reduce Hospitalization for Children With Isolated Skull Fractures
- PMID: 27244848
- PMCID: PMC4894255
- DOI: 10.1542/peds.2015-3370
A QI Initiative to Reduce Hospitalization for Children With Isolated Skull Fractures
Abstract
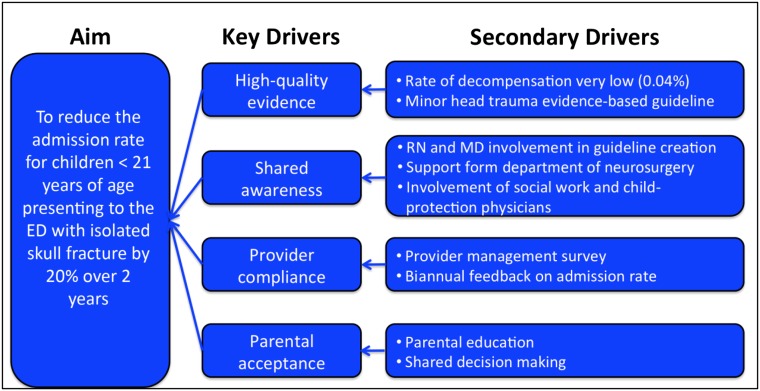
Background and objective: Although children with isolated skull fractures rarely require acute interventions, most are hospitalized. Our aim was to safely decrease the hospitalization rate for children with isolated skull fractures.
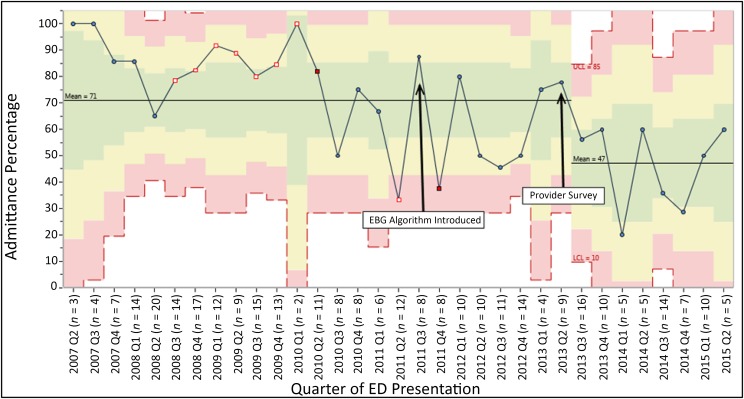
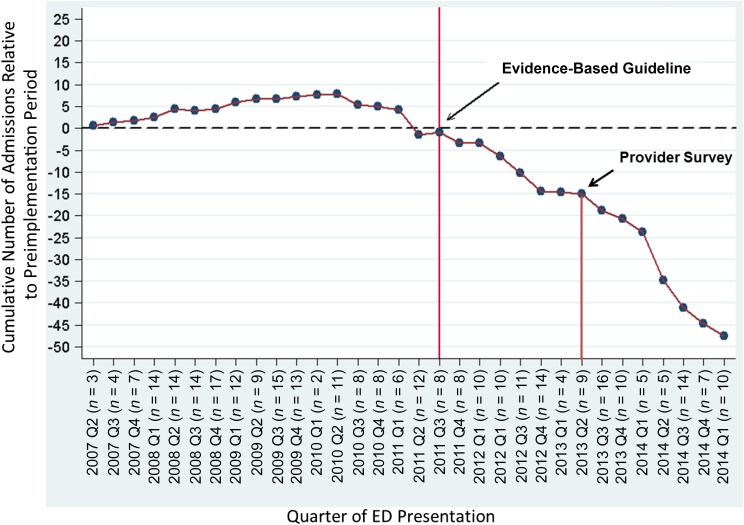
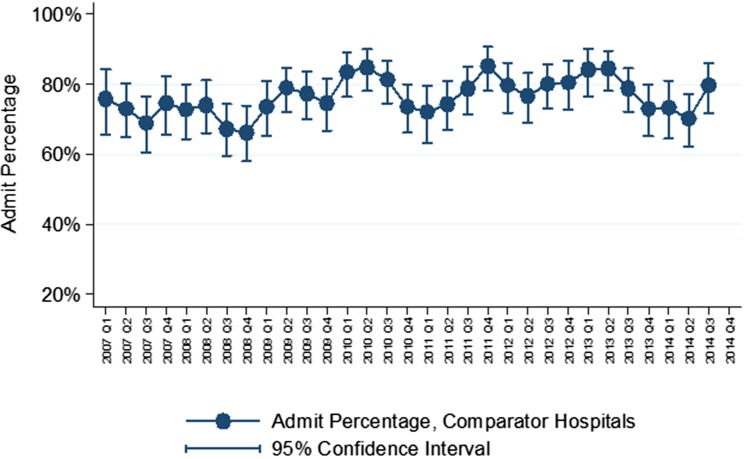
Methods: We designed and executed this multifaceted quality improvement (QI) initiative between January 2008 and July 2015 to reduce hospitalization rates for children ≤21 years old with isolated skull fractures at a single tertiary care pediatric institution. We defined an isolated skull fracture as a skull fracture without intracranial injury. The QI intervention consisted of 2 steps: (1) development and implementation of an evidence-based guideline, and (2) dissemination of a provider survey designed to reinforce guideline awareness and adherence. Our primary outcome was hospitalization rate and our balancing measure was hospital readmission within 72 hours. We used standard statistical process control methodology to assess change over time. To assess for secular trends, we examined admission rates for children with an isolated skull fracture in the Pediatric Health Information System administrative database.
Results: We identified 321 children with an isolated skull fracture with a median age of 11 months (interquartile range 5-16 months). The baseline admission rate was 71% (179/249, 95% confidence interval, 66%-77%) and decreased to 46% (34/72, 95% confidence interval, 35%-60%) after implementation of our QI initiative. No child was readmitted after discharge. The admission rate in our secular trend control group remained unchanged at 78%.
Conclusions: We safely reduced the hospitalization rate for children with isolated skull fractures without an increase in the readmissions.
Copyright © 2016 by the American Academy of Pediatrics.
Conflict of interest statement
Figures
References
-
- Centers for Disease Control and Prevention, National Center for Injury Prevention and Control Traumatic brain injury in the United States: Assessing outcomes in children. Available at: www.cdc.gov/ncipc/tbi/tbi_report/index.htm. Accessed July 1, 2013
-
- Rutland-Brown W, Langlois JA, Thomas KE, Xi YL. Incidence of traumatic brain injury in the United States, 2003. J Head Trauma Rehabil. 2006;21(6):544–548 - PubMed
-
- Schutzman SA, Greenes DS. Pediatric minor head trauma. Ann Emerg Med. 2001;37(1):65–74 - PubMed
-
- Schneier AJ, Shields BJ, Hostetler SG, Xiang H, Smith GA. Incidence of pediatric traumatic brain injury and associated hospital resource utilization in the United States. Pediatrics. 2006;118(2):483–492 - PubMed
-
- Quayle KS, Jaffe DM, Kuppermann N, et al. Diagnostic testing for acute head injury in children: when are head computed tomography and skull radiographs indicated? Pediatrics. 1997;99(5). Available at: www.pediatrics.org/cgi/content/full/99/5/e11 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
