

Prevalence of weakness and its relationship with limitations based on the Foundations for the National Institutes for Health project: data from the Health and Retirement Study
- PMID: 27245209
- PMCID: PMC5052111
- DOI: 10.1038/ejcn.2016.90
Prevalence of weakness and its relationship with limitations based on the Foundations for the National Institutes for Health project: data from the Health and Retirement Study
Abstract
Background/objectives: The objectives of this study were to determine the prevalence of muscle weakness using the two 2014 Foundation for the National Institutes of Health (FNIH) Sarcopenia Project criteria and its relationship with physical limitations, basic activities of daily living (ADL) and instrumental ADL.
Subjects/methods: We performed a cross-sectional analysis of community-dwelling adults from the Health and Retirement Study 2006-2008 and identified a subsample of 5092 adults aged ⩾60 years with grip strength (GS) data. Self-reported physical limitations, basic ADL and instrumental ADL were assessed. Criteria for GS (men<26 kg; women <16 kg) and GS adjusted for body mass index (GS/BMI; men <1.0; women <0.56) were applied to the sample. We determined the prevalence of muscle weakness in each sex. Multivariable logistic regression was used to calculate the association of physical limitations, basic ADL and instrument ADL with weakness definitions in each sex.
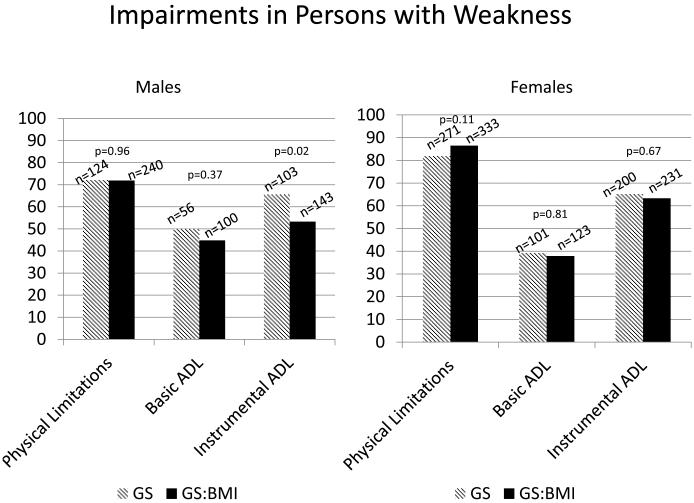
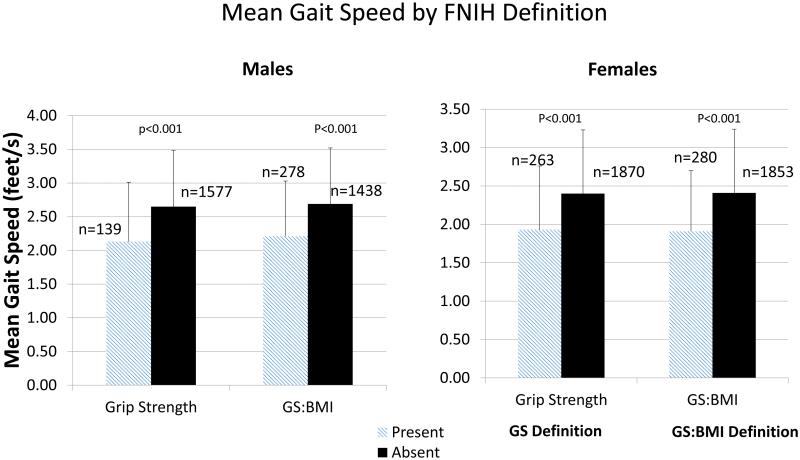
Results: Mean age was 72.1 years (54.9% female). Mean GS was 38.3 and 22.9 kg and mean BMI was 29 kg/m2, respectively, in men and women. Weakness prevalence using GS and GS:BMI definitions were 7.8 and 15.2 (P<0.001), respectively, in men and 11.4 and 13.3% (P=0.04) in women. Overall prevalence of physical limitations, basic ADL limitations and instrumental ADL limitations was 52.9, 28.1 and 35.9%, respectively. In those with weakness, prevalence of physical limitations, basic ADL and instrumental ADL was 78.5, 42.3 and 65.3%, respectively, using the GS definition, and 79.7, 40.7 and 58.8%, respectively, using the GS/BMI definition. GS and the GS/BMI definitions of weakness were strongly associated with physical limitations (odds ratio (OR) 2.19 (95% confidence interval (CI): (1.67-2.87)) and 2.52 (2.01-3.17)), basic ADL (OR 1.59 (1.22-2.07) and 1.66 (1.32-2.07)) and instrumental ADLs (OR 1.98 (1.28-2.54) and 1.78 (1.44-2.20)).
Conclusions: The new FNIH guidelines for weakness are associated with higher prevalence of physical limitations, basic ADL impairments and instrumental ADL impairments as compared with individuals without weakness.
Figures
References
-
- Newman AB, Kupelian V, Visser M, Simonsick EM, Goodpaster BH, Kritchevsky SB, et al. Strength, but not muscle mass, is associated with mortality in the health, aging and body composition study cohort. J. Gerontol. A. Biol. Sci. Med. Sci. 2006;61(1):72–77. e-pub ahead of print 2006/02/04. - PubMed
-
- Visser M, Kritchevsky SB, Goodpaster BH, Newman AB, Nevitt M, Stamm E, et al. Leg muscle mass and composition in relation to lower extremity performance in men and women aged 70 to 79: The health, aging and body composition study. J. Am. Geriatr. Soc. 2002;50(5):897–904. doi: 10.1046/j.1532-5415.2002.50217.x. - PubMed
-
- Studenski SA, Peters KW, Alley DE, Cawthon PM, McLean RR, Harris TB, et al. The FNIH sarcopenia project: rationale, study description, conference recommendations, and final estimates. J. Gerontol. A. Biol. Sci. Med. Sci. 2014;69(5):547–558. e-pub ahead of print 2014/04/17; doi: 10.1093/gerona/glu010. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
