

Headache, depression and anxiety: associations in the Eurolight project
- PMID: 27245683
- PMCID: PMC4887397
- DOI: 10.1186/s10194-016-0649-2
Headache, depression and anxiety: associations in the Eurolight project
Abstract
Background: Headache disorders and psychiatric disorders are both common, while evidence, mostly pertaining to migraine, suggests they are comorbid more often than might be expected by chance. There are good reasons for establishing whether they are: symptoms of comorbid illnesses may summate synergistically; comorbidities hinder management, negatively influencing outcomes; high-level comorbidity indicates that, where one disease occurs, the other should be looked for. The Eurolight project gathered population-based data on these disorders from 6624 participants.
Methods: Eurolight was a cross-sectional survey sampling from the adult populations (18-65 years) of 10 EU countries. We used data from six. The questionnaire included headache-diagnostic questions based on ICHD-II, the Headache-Attributed Lost Time (HALT) questionnaire, and HADS for depression and anxiety. We estimated odds ratios (ORs) to show associations between migraine, tension-type headache (TTH) or probable medication-overuse headache (pMOH) and depression or anxiety.
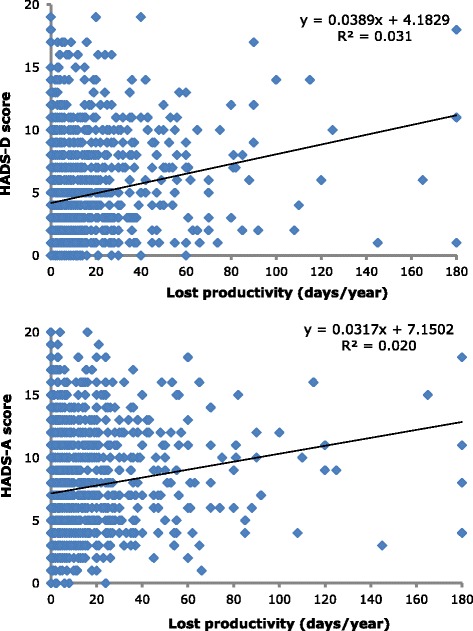
Results: pMOH was most strongly associated with both psychiatric disorders: for depression, ORs (vs no headache) were 5.5 [2.2-13.5] (p < 0.0001) in males, 5.5 [2.9-10.5] (p < 0.0001) in females; for anxiety, ORs were 10.4 [4.9-21.8] (p < 0.0001) and 7.1 [4.5-11.2] (p < 0.0001). Migraine was also associated with both: for depression, ORs were 2.1 [1.3-3.4] (p = 0.002) and 1.8 [1.1-3.1] (p = 0.030); for anxiety 4.2 [2.8-6.3] (p < 0.0001) and 2.4 [1.7-3.4] (p < 0.0001). TTH showed associations only with anxiety: ORs 2.5 [1.7-3.7] (p < 0.0001) for males, 1.5 [1.1-2.1] (p = 0.021) for females. Participants with migraine carried 19.1 % probability of comorbid anxiety, 6.9 % of depression and 5.1 % of both, higher than the representative general-population sample (14.3, 5.6 and 3.8 %). Probabilities in those with MOH were 38.8, 16.9 and 14.4 %; in TTH, they did not exceed those of the whole sample. Comorbid psychiatric disorder did not add to headache-attributed productive time losses, but weak associations existed (R (2) = 0.020-0.082) for all headache types between lost productive time and probabilities of depression and, less so, anxiety.
Conclusion: In this large study we confirmed that depression and especially anxiety are comorbid more than by chance with migraine, and showed the same is true, but more strongly, with MOH. Arguably, migraine patients and, more certainly, MOH patients should be screened with HADS in pursuit of best outcomes.
Keywords: Anxiety; Associations; Comorbidity; Depression; Eurolight project; Europe; Global Campaign against Headache; Headache; Medication-overuse headache; Migraine; Public health; Tension-type headache.
Figures
References
-
- Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, Shibuya K, Salomon JA, Abdalla S, Aboyans V, Abraham J, Ackerman I, Aggarwal R, Ahn SY, Ali MK, Alvarado M, Anderson HR, Anderson LM, Andrews KG, Atkinson C, Baddour LM, Bahalim AN, Barker-Collo S, Barrero LH, Bartels DH, Basáñez MG, Baxter A, Bell ML, Benjamin EJ, Bennett D, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2163–2196. doi: 10.1016/S0140-6736(12)61729-2. - DOI - PMC - PubMed
-
- Vos T, Barber RM, Bell B, Bertozzi-Villa A, Biryukov S, Bolliger I, Charlson F, Davis A, Degenhardt L, Dicker D, Duan L, Erskine H, Feigin VL, Ferrari AJ, Fitzmaurice C, Fleming T, Graetz N, Guinovart C, Haagsma J, Hansen GM, Hanson SW, Heuton KR, Higashi H, Kassebaum N, Kyu H, Laurie E, Liang X, Lofgren K, Lozano R, MacIntyre MF, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386:743–800. doi: 10.1016/S0140-6736(15)60692-4. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
