

Development and clinical application of an integrative genomic approach to personalized cancer therapy
- PMID: 27245685
- PMCID: PMC4888213
- DOI: 10.1186/s13073-016-0313-0
Development and clinical application of an integrative genomic approach to personalized cancer therapy
Abstract
Background: Personalized therapy provides the best outcome of cancer care and its implementation in the clinic has been greatly facilitated by recent convergence of enormous progress in basic cancer research, rapid advancement of new tumor profiling technologies, and an expanding compendium of targeted cancer therapeutics.
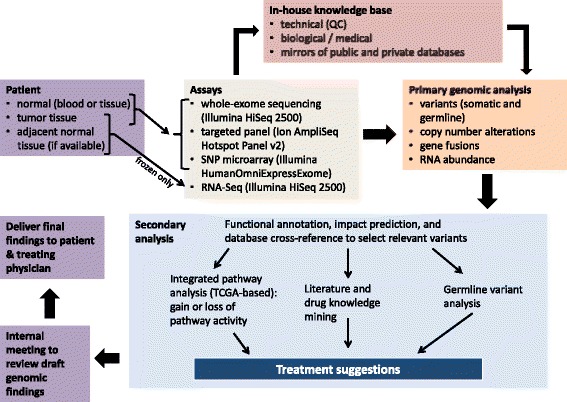
Methods: We developed a personalized cancer therapy (PCT) program in a clinical setting, using an integrative genomics approach to fully characterize the complexity of each tumor. We carried out whole exome sequencing (WES) and single-nucleotide polymorphism (SNP) microarray genotyping on DNA from tumor and patient-matched normal specimens, as well as RNA sequencing (RNA-Seq) on available frozen specimens, to identify somatic (tumor-specific) mutations, copy number alterations (CNAs), gene expression changes, gene fusions, and also germline variants. To provide high sensitivity in known cancer mutation hotspots, Ion AmpliSeq Cancer Hotspot Panel v2 (CHPv2) was also employed. We integrated the resulting data with cancer knowledge bases and developed a specific workflow for each cancer type to improve interpretation of genomic data.
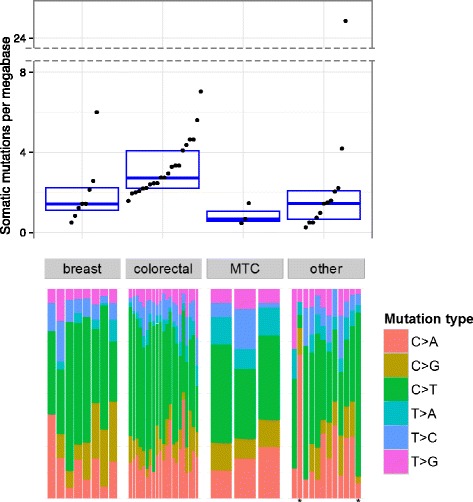
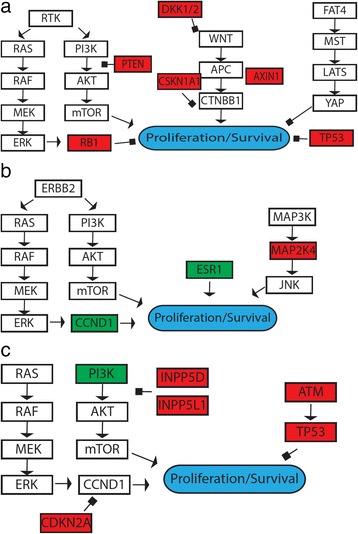
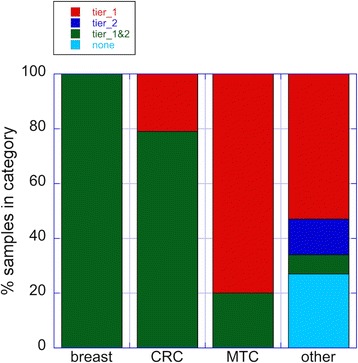
Results: We returned genomics findings to 46 patients and their physicians describing somatic alterations and predicting drug response, toxicity, and prognosis. Mean 17.3 cancer-relevant somatic mutations per patient were identified, 13.3-fold, 6.9-fold, and 4.7-fold more than could have been detected using CHPv2, Oncomine Cancer Panel (OCP), and FoundationOne, respectively. Our approach delineated the underlying genetic drivers at the pathway level and provided meaningful predictions of therapeutic efficacy and toxicity. Actionable alterations were found in 91 % of patients (mean 4.9 per patient, including somatic mutations, copy number alterations, gene expression alterations, and germline variants), a 7.5-fold, 2.0-fold, and 1.9-fold increase over what could have been uncovered by CHPv2, OCP, and FoundationOne, respectively. The findings altered the course of treatment in four cases.
Conclusions: These results show that a comprehensive, integrative genomic approach as outlined above significantly enhanced genomics-based PCT strategies.
Keywords: Cancer; Clinical application; Genomics; Personalized medicine.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
