

Initiation of and long-term adherence to secondary preventive drugs after acute myocardial infarction
- PMID: 27246583
- PMCID: PMC4886431
- DOI: 10.1186/s12872-016-0283-6
Initiation of and long-term adherence to secondary preventive drugs after acute myocardial infarction
Abstract
Background: Secondary preventive drug therapy following acute myocardial infarction (AMI) is recommended to reduce the risk of new cardiovascular events. The aim of this nationwide cohort study was to examine the initiation and long-term use of secondary preventive drugs after AMI.
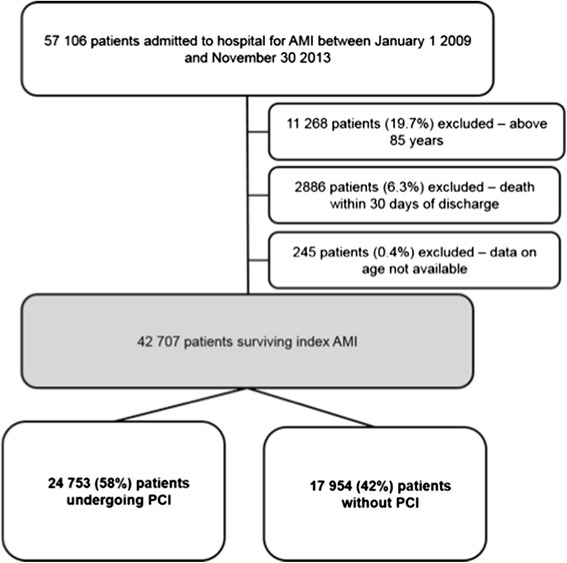
Methods: The prescription of drugs in 42,707 patients < 85 years discharged alive from hospital after AMI in 2009-2013 was retrieved by linkage of the Norwegian Patient Register, the Norwegian Prescription Database, and the Norwegian Cause of Death Registry. Patients were followed for up to 24 months.
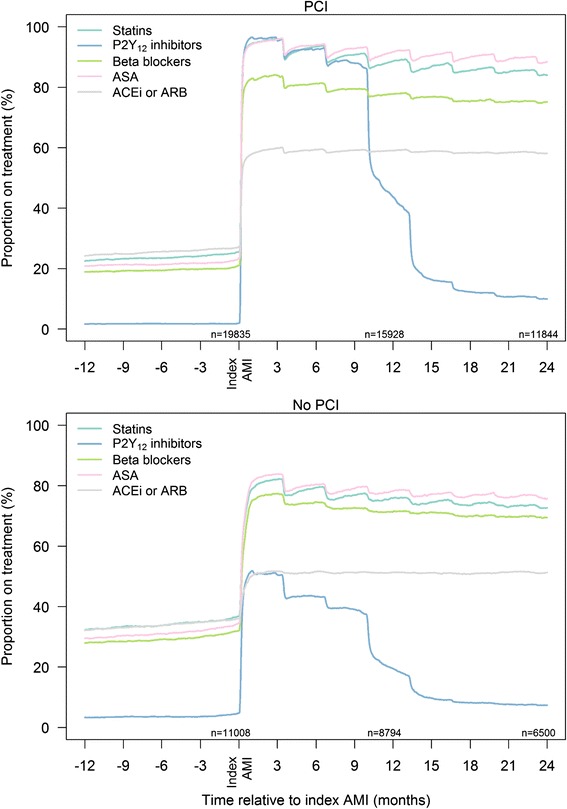
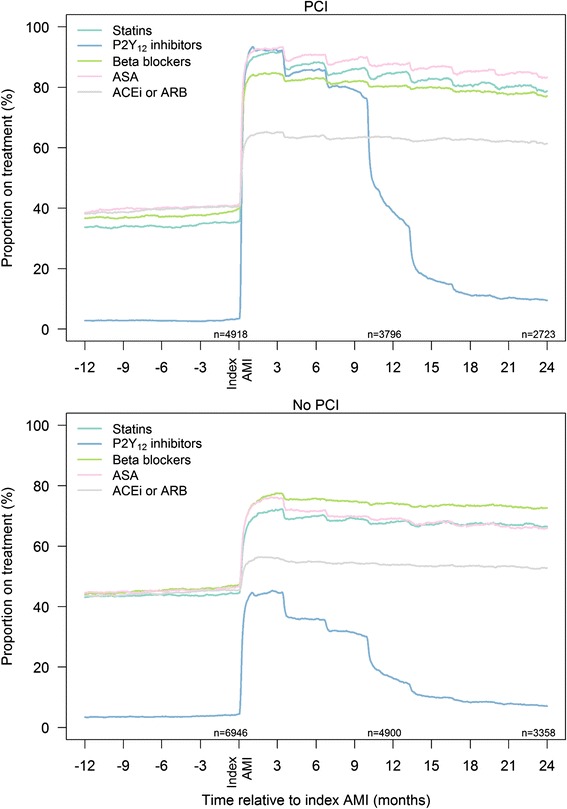
Results: The majority of patients were discharged on single or dual antiplatelet therapy (91 %), statins (90 %), beta-blockers (82 %), and angiotensin-converting enzyme inhibitors (ACEI)/angiotensin receptor II blockers (ARB) (60 %). Patients not undergoing percutaneous coronary intervention (PCI) (42 %) were less likely to be prescribed secondary preventive drugs compared with patients undergoing PCI. This was particular the case for dual antiplatelet therapy (43 % vs. 87 %). The adherence to prescribed drugs was high: 12 months after index AMI, 84 % of patients were still on aspirin, 84 % on statins, 77 % on beta-blockers and 57 % on ACEI/ARB. Few drug and dose adjustments were made during follow-up.
Conclusion: Guideline-recommended secondary preventive drugs were prescribed to most patients discharged from hospital after AMI, but the percentage receiving such therapy was significantly lower in non-PCI patients. The long-time adherence was high, but few drug adjustments were performed during follow-up. More attention is needed to secondary preventive drug therapy in AMI patients not undergoing PCI.
Keywords: Acute myocardial infarction; Medication adherence; Secondary prevention.
Figures

References
-
- Patient statistics, 2014. Available at: https://www.ssb.no/en/helse/statistikker/pasient. Accessed 1 Oct 2015.
-
- Task Force for Diagnosis and Treatment of Non-ST-Segment Elevation Acute Coronary Syndromes of European Society of Cardiology, Bassand JP, Hamm CW, Ardissino D, Boersma E, Budaj A, et al. Guidelines for the diagnosis and treatment of non-ST-segment elevation acute coronary syndromes. Eur Heart J. 2007;28:1598–660. - PubMed
-
- Hamm CW, Bassand JP, Agewall S, Bax J, Boersma E, Bueno H, Caso P, Dudek D, Gielen S, Huber K, Ohman M, Petrie MC, Sonntag F, Uva MS, Storey RF, Wijns W, Zahger D, ESC Committee for Practice Guidelines ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: The task force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European Society of Cardiology. Eur Heart J. 2011;32:2999–54. doi: 10.1093/eurheartj/ehr236. - DOI - PubMed
-
- Van de Werf F, Bax J, Betriu A, Blomstrom-Lundqvist C, Crea F, Falk V, Filippatos G, Fox K, Huber K, Kastrati A, Rosengren A, Steg PG, Tubaro M, Verheugt F, Weidinger F, Weis M, ESC Committee for Practice Guidelines (CPG) Management of acute myocardial infarction in patients presenting with persistent ST-segment elevation: the Task Force on the Management of ST-Segment Elevation Acute Myocardial Infarction of the European Society of Cardiology. Eur Heart J. 2008;29:2909–45. doi: 10.1093/eurheartj/ehn416. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
